
Rationale and Objectives
To prospectively assess the incremental value of diffusion-weighted imaging (DWI) combined with T2-weighted images (T2WI) in determining the T stage of bladder cancer by using pathologic findings as the reference standard.
Materials and Methods
This study is approved by the institutional review board; informed consent was waived. The study includes 362 patients (age range, 48–87 years; mean, 71 years) who underwent 3.0-T magnetic resonance imaging and histologic examination. Three observers with varying experience levels reviewed the T2WI data alone, DWI data alone, and combined T2WI and DWI data. Sensitivity, specificity, accuracy, and area under curve (AUC) were determined with the Z test after adjusting for data clustering.
Results
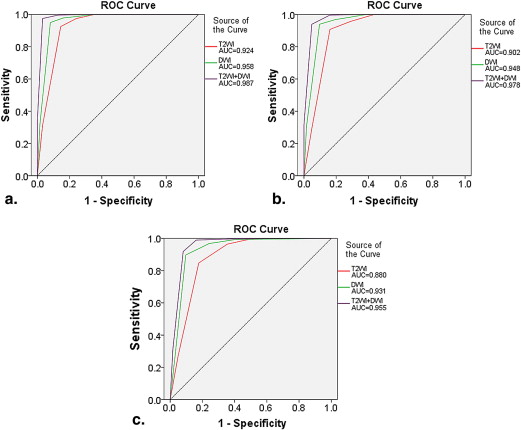
For differentiating Tis to T1 tumors from T2 to T4 tumors, the AUCs for T2WI and DWI (0.97 for observer 1 and 0.96 for observer 2) were greater than those for the DWI alone (0.92 for observer 1 and 0.90 for observer 2) ( P < .05). Observer 3 had similar AUCs for T2WI and DWI compared to DWI alone. The accuracy of T2WI and DWI (observer 1, 98%; observer 2, 96%; observer 3, 92%) was greater than that of DWI alone (observer 1, 92%; observer 2, 90%; observer 3, 87%) for all observers ( P < .05). The specificity of T2WI and DWI (observer 1, 100%; observer 2, 98%; observer 3, 93%) was greater than that of DWI alone (observer 1, 92%; observer 2, 90%; observer 3, 87%) for all observers ( P < .05). Sensitivity was not improved even when T2WI and DWI were used. For differentiating Tis to T2 Tumors from T3 to T4 Tumors, the overall accuracy, specificity, and AUC for diagnosing T2 or higher stages were not significantly improved by combiningT2WI and DWI.
Conclusions
T2WI combined with DWI can be a reliable sequence for preoperative evaluation of T stage urinary bladder cancer. It is particularly more useful in differentiating T1 or lower tumors from T2 or higher tumors compared to DWI alone.
Bladder cancer (BC) is a common type of cancer that can cause substantial morbidity and mortality among both men and women. BC causes 14,880 deaths per year in the United States . Clinical management of urinary BC is determined primarily on the basis of distinguishing superficial tumors (stage T1 or lower) from muscle-invasive tumors (stage T2 or higher), as proper treatment options differ considerably between these two stages. Superficial tumors are treated with transurethral resection (TUR) with or without adjuvant intravesical chemotherapy or photodynamic therapy , whereas invasive tumors are treated with radical cystectomy, radiation therapy, chemotherapy, or a combination . Therefore, preoperative imaging studies play an important diagnostic role in precisely differentiating between the two categories of BC.
Computed tomography (CT), as the preferred method for the staging of BC, has high accuracy in the diagnosis of BC . However, it cannot reliably determine the depth of tumor invasion into the bladder wall, the involvement of adjacent organs, or the presence of nodal disease . In addition, the high radiation exposure and the need for an ionizing contrast agent encourage the use of other imaging modalities for muscle-invasive BC (MIBC) staging . The reported magnetic resonance (MR) staging accuracy for bladder carcinoma ranges from 72% to 96% . Staging is improved with gadolinium enhancement . However, accurate staging with imaging techniques is difficult because of the thinness of the bladder wall, which accounts for the difficulty in distinguishing superficial invasion (pT2a) from deep muscle invasion (pT2 b) and deep muscle invasion from minor tumor extension into perivesical fat (pT3a) .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Patients
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
MRI Examination
Get Radiology Tree app to read full this article<
MR Image Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
T Staging for Bladder Cancer
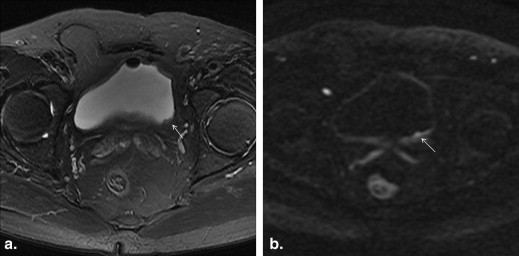
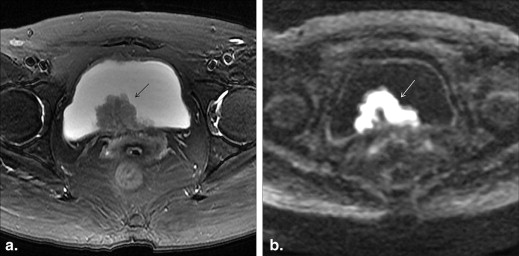
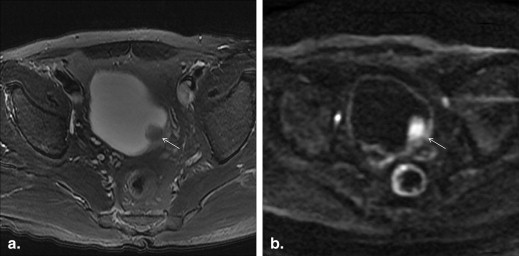
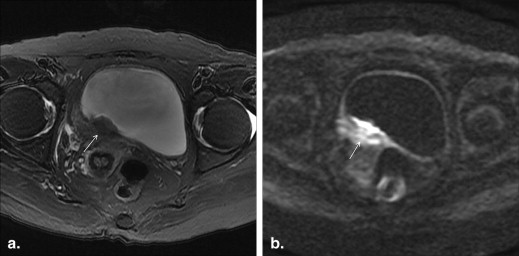
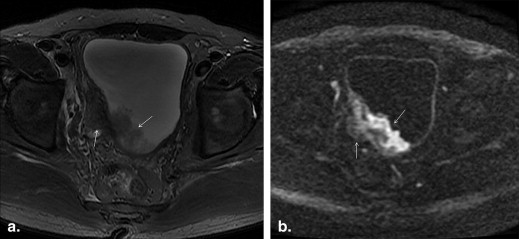
Stage Description N Staging Definition DWI T2WI Tis Carcinoma in situ 257 A thin, flat, high SI area corresponding to the tumor or a high SI tumor with a low SI submucosal stalk or a thickened submucosa Low SI line was present Ta Papillary noninvasive tumor T1 Tumor invades subepithelial connective tissue T2a Tumor invades superficial muscle 25 A high SI tumor without a submucosal stalk and with a smooth tumor margin The low SI line was disrupted focally in the region underlying the tumor T2 b Tumor invades deep muscle T3a Tumor invades perivesical tissue microscopically 40 Extension into the perivesical fat with an irregular margin T3 b Tumor invades perivesical tissue macroscopically T4a Tumor invades prostate, uterus, or vagina 22 Extension into adjacent organs T4 b Tumor invades pelvic or abdominal wall
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Result
Tumor Characteristics
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Comparison of Accuracy of Imaging Acquisitions
Get Radiology Tree app to read full this article<
Table 2
AUCs of Three Data Sets for Differentiating Stage Tis to T1 Tumors from T2 to T4 Tumors for Three Observers
Observer T2WI Alone DWI Alone T2WI and DWI_P_ Value ∗ P Value † 1 0.90 (0.86–0.94) 0.92 (0.88–0.96) 0.97 (0.95–1.00) <.0001 .001 2 0.86 (0.82–0.91) 0.90 (0.77–0.94) 0.96 (0.93–0.99) <.0001 .014 3 0.85 (0.81–0.80) 0.90 (0.86–0.94) 0.95 (0.93–0.98) <.0001 .184
Data in parentheses are 95% confidence intervals.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
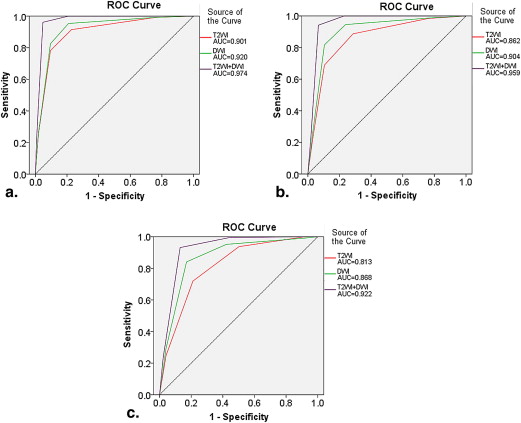
Table 3
AUCs of Three Data Sets for Differentiating Stage Tis to T2 Tumors from T3 to T4 Tumors for Three Observers
Observer T2WI Alone DWI Alone T2WI and DWI_P_ Value ∗ P Value † 1 0.92 (0.88–0.97) 0.96 (0.92–0.99) 0.99 (0.98–1.00) .079 .151 2 0.90 (0.85–0.96) 0.95 (0.91–0.99) 0.98 (0.96–1.00) .051 .164 3 0.88 (0.82–0.94) 0.93 (0.89–0.98) 0.96 (0.92–0.99) .128 .135
Data in parentheses are 95% confidence intervals.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 4
Comparison of Three Data Sets for Differentiating Stage Tis to T1 Tumors from T2 to T4 Tumors for Three Observers
Parameter T2WI Alone DWI Alone T2WI and DWI_P_ Value ∗ P Value † Reader 1 Sensitivity 91 (96/105) 91 (96/105) 94 (99/105) .297 .297 Specificity 79 (203/257) 92 (236/257) 100 (257/257) <.001 <.001 Accuracy 83 (299/362) 92 (332/362) 98 (356/362) <.001 <.001 Reader 2 Sensitivity 87 (91/105) 89 (93/105) 92 (97/105) .13 .241 Specificity 73 (188/257) 91 (234/257) 98 (252/257) <.001 <.001 Accuracy 77 (279/362) 90 (327/362) 96 (349/362) <.001 <.001 Reader 3 Sensitivity 81 (85/105) 86 (90/105) 89 (93/105) .089 .340 Specificity 71 (182/257) 88 (226/257) 93 (239/257) <.001 <.001 Accuracy 74 (267/362) 87 (316/362) 92 (332/362) <.001 <.001
Data are percentages, with numbers used to calculate percentages in parentheses.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 5
Comparison of Three Data Sets for Differentiating Stage Tis to T2 Tumors from T3 to T4 Tumors for Three Observers
Parameter T2WI Alone DWI Alone T2WI and DWI_P_ Value ∗ P Value † Reader 1 Sensitivity 85 (53/62) 88 (55/62) 92 (57/62) .198 .381 Specificity 94 (265/282) 96 (271/282) 100 (282/282) <.001 <.001 Accuracy 92 (318/344) 95 (326/344) 99 (339/344) <.001 .005 Reader 2 Sensitivity 81 (50/62) 85 (53/62) 89 (55/62) .159 .395 Specificity 91 (257/282) 95 (268/282) 97 (274/282) .002 .138 Accuracy 74 (307/344) 93 (321/344) 96 (329/344) <.001 .121 Reader 3 Sensitivity 72 (45/62) 83 (51/62) 87 (54/62) .036 .309 Specificity 85 (240/282) 91 (257/282) 94 (265/282) <.001 .131 Accuracy 83 (285/344) 90 (308/344) 93 (319/344) <.001 .090
Data are percentages, with numbers used to calculate percentages in parentheses.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Comparison of Observer Accuracy for T2WI and DWI
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Hadjiiski L., Chan H.P., Caoili E.M., et. al.: Auto-initialized cascaded level set (AI-CALS) segmentation of bladder lesions on multidetector row CT urography. Acad Radiol 2013; 20: pp. 148-155.
2. Josephson D., Pasin E., Stein J.P.: Superficial bladder cancer. II. Management. Exp Rev Anticancer Ther 2007; 7: pp. 567-581.
3. Sherif A., Jonsson M.N., Wiklund N.P.: Treatment of muscle-invasive bladder cancer. Expert Rev Anticancer Ther 2007; 7: pp. 1279-1283.
4. Knox M.K., Cowan N.C., Rivers-Bowerman M.D., et. al.: Evaluation of multidetector computed tomography urography and ultrasonography for diagnosing bladder cancer. Clin Radiol 2008; 63: pp. 1317-1325.
5. Razavi S.A., Sadigh G., Kelly A.M., et. al.: Comparative effectiveness of imaging modalities for the diagnosis of upper and lower urinary tract malignancy: a critically appraised topic. Acad Radiol 2012; 19: pp. 1134-1140.
6. Setty B.N., Holalkere N.S., Sahani D.V., et. al.: State-of-the-art cross-sectional imaging in bladder cancer. Curr Probl Diagn Radiol 2007; 36: pp. 83-96.
7. Baltaci S., Resorlu B., Yagci C., et. al.: Computerized tomography for detecting perivesical infiltration and lymph node metastasis in invasive bladder carcinoma. Urol Int 2008; 81: pp. 399-402.
8. Totaro A., Pinto F., Brescia A., et. al.: Imaging in bladder cancer: present role and future perspectives. Urol Int 2010; 85: pp. 373-380.
9. Husband J.E.S., Olliff J.F.C., Williams M.P., et. al.: Bladder cancer: staging with CT and MR imaging. Radiology 1989; 173: pp. 435-440.
10. Akmangit I., Lakadamyali H., Oto A., et. al.: Staging of urinary bladder tumours with CT and MRI. Turk J Diagn Intervent Radiol 2003; 9: pp. 63-69.
11. Kundra V., Siverman P.M.: Imaging in oncology from the University of Texas M.D. Anderson Cancer Center. AJR Am J Roentgenol 2003; 180: pp. 1045-1054.
12. Tillou X., Grardel E., Fourmarier M., et. al.: Can MRI be used to distinguish between superficial and invasive transitional cell bladder cancer?. Prog Urol 2008; 18: pp. 440-444.
13. Barentsz J.O., Jager G.J., van Vierzen P.B., et. al.: Staging urinary bladder cancer after transurethral biopsy: value of fast dynamic contrast-enhanced MR imaging. Radiology 1996; 201: pp. 185-193.
14. Barentsz J.O., Jager G.J., Witjes J.A., et. al.: Primary staging of urinary bladder carcinoma: the role of MR imaging and a comparison with CT. Eur Radiol 1996; 6: pp. 134-139.
15. Takeuchi M., Suzuki T., Sasaki S., et. al.: Clinicopathologic significance of high signal intensity on diffusion-weighted MR imaging in the ureter, urethra, prostate and bone of patients with bladder cancer. Acad Radiol 2012; 19: pp. 827-833.
16. El-Assmy A., Abou-El-Ghar M.E., Mosbah A., et. al.: Bladder tumour staging: comparison of diffusion- and T2-weighted MR imaging. Eur Radiol 2009; 19: pp. 1575-1581.
17. Takeuchi M., Sasaki S., Ito M., et. al.: Urinary bladder cancer: diffusion-weighted MR imaging–accuracy for diagnosing T stage and estimating histologic grade. Radiology 2009; 251: pp. 112-121.
18. Watanabe H., Kanematsu M., Kondo H., et. al.: Preoperative T staging of urinary bladder cancer: does diffusion-weighted MRI have supplementary value?. AJR Am J Roentgenol 2009; 192: pp. 1361-1366.
19. Sobin L.H.Wittekind C.H.International Union Against Cancer (UICC): TNM classification of malignant tumors.1997.Wiley-LissNew York, NY:pp. 170-173.
20. Fisher M.R., Hricak H., Tanagho E.A.: Urinary bladder MR imaging. II. Neoplasm. Radiology 1985; 157: pp. 471-477.
21. Buy J.N., Moss A.A., Guinet C., et. al.: MR staging of bladder carcinoma: correlation with pathologic findings. Radiology 1988; 169: pp. 695-700.
22. Rholl K.S., Lee J.K., Heiken J.P., et. al.: Primary bladder carcinoma: evaluation with MR imaging. Radiology 1987; 163: pp. 117-121.
23. Narumi Y., Kadota T., Inoue E., et. al.: Bladder wall morphology: in vitro MR imaging-histopathologic correlation. Radiology 1993; 187: pp. 151-155.
24. Matsuki M., Inada Y., Tatsugami F., et. al.: Diffusion-weighted MR imaging for urinary bladder carcinoma: initial results. Eur Radiol 2007; 17: pp. 201-204.
25. Zhou X., Obuchowski N., McClish D.: Comparing the accuracy of two diagnostic tests.Statistical methods in diagnostic medicine.2002.WileyNew York, NY:pp. 171-176.
26. Park M.J., Cha E.S., Kang B.J., et. al.: The role of diffusion-weighted imaging and the apparent diffusion coefficient (ADC) values for breast tumors. Kor J Radiol 2007; 8: pp. 390-396.
27. Baltzer P.A., Benndorf M., Dietzel M., et. al.: Sensitivity and specificity of unenhanced MR mammography (DWI combined with T2-weighted TSE imaging, ueMRM) for the differentiation of mass lesions. Eur Radiol 2010; 20: pp. 1101-1110.
28. Baltzer P.A., Renz D.M., Herrmann K.H., et. al.: Diffusion-weighted imaging (DWI) in MR mammography (MRM): clinical comparison of echo planar imaging (EPI) and half-Fourier single-shot turbo spin echo (HASTE) diffusion techniques. Eur Radiol 2009; 19: pp. 1612-1620.
29. Tekes A., Kamel I., Imam K., et. al.: Dynamic MRI of bladder cancer: evaluation of staging accuracy. AJR Am J Roentgenol 2005; 184: pp. 121-127.
30. Hayashi N., Tochigi H., Shiraishi T., et. al.: A new staging criterion for bladder carcinoma using gadolinium-enhanced magnetic resonance imaging with an endorectal surface coil: a comparison with ultrasonography. BJU Int 2000; 85: pp. 32-36.
31. Narumi Y., Kadota T., Inoue E., et. al.: Bladder tumors: staging with gadolinium-enhanced oblique MR imaging. Radiology 1993; 187: pp. 145-150.