
Rationale and Objectives
The objective of this study was to evaluate the association of communication practices with timely follow-up of screening mammograms read as Breast Imaging Reporting and Data Systems (BI-RADS) 0 in the Population-based Research Optimizing Screening through Personalized Regimens (PROSPR) consortium.
Materials and Methods
A radiology facility survey was conducted in 2015 with responses linked to screening mammograms obtained in 2011–2014. We considered timely follow-up to be within 15 days of the screening mammogram. Generalized estimating equation models were used to evaluate the association between modes of communication with patients and providers and timely follow-up, adjusting for PROSPR site, patient age, and race and ethnicity.
Results
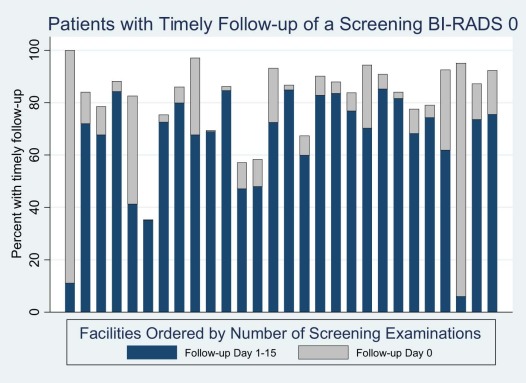
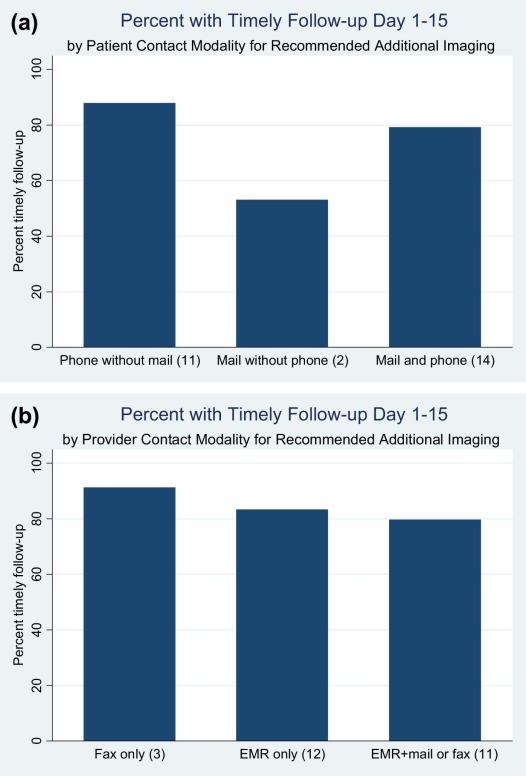
The analysis included 34,680 mammography examinations with a BI-RADS 0 assessment among 28 facilities. Across facilities, 85.6% of examinations had a follow-up within 15 days. Patients in a facility where routine practice was to contact the patient by phone if follow-up imaging was recommended were more likely to have timely follow-up (odds ratio [OR] 4.63, 95% confidence interval [CI] 2.76–7.76), whereas standard use of mail was associated with reduced timely follow-up (OR 0.47, 95% CI 0.30–0.75). Facilities that had standard use of electronic medical records to report the need for follow-up imaging to a provider had less timely follow-up (OR 0.56, 95% CI 0.35–0.90). Facilities that routinely contacted patients by mail if they missed a follow-up imaging visit were more likely to have timely follow-up (OR 1.65, 95% CI 1.02–2.69).
Conclusions
Our findings support the value of telephone communication to patients in relation to timely follow-up. Future research is needed to evaluate the role of communication in completing the breast cancer screening episode.
Introduction
Mammography screening reduces breast cancer mortality among women aged 40–74 years . Progression through the screening process, from initial screening, through follow-up of abnormal results, to treatment, can fail at multiple points in the screening episode . Lack of effective communication between facilities, providers, and patients may delay follow-up and lead to adverse health outcomes, including anxiety, delay in diagnosis, and widening of cancer outcome disparities .
Mode of communication can impact timely follow-up of abnormal mammograms. Commonly used modes of communicating mammography results to patients include verbal communication (including in-person communication, by telephone, and leaving a voice message) and written communication by conventional mail or through a patient portal to the electronic medical record (EMR). In a study among women of diverse ethnicity who had a screening mammogram and a Breast Imaging Reporting and Data Systems (BI-RADS) 0 result, discussion of results with a provider was associated with more timely follow-up, although this finding did not persist on multivariate analysis controlling for insurance status . Communication factors such as patients asking questions, receiving next-step information, and being told that follow-up is needed have also been associated with timely follow-up of an abnormal mammogram .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and Methods
Get Radiology Tree app to read full this article<
Survey Content and Coding of Responses
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Survey Protocol
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Facilities, Screening Examinations (2011–2014), BI-RADS 0, and Timely Follow-up
Health-care Setting (PROSPR Center) Number of Facilities Screening Examinations Number of Months of Examinations Included BI-RADS 0
n (%) Follow-up, ≤15 d
n (%) \* Follow-up, Same Day
n (%) Follow-up, Days 1–15
n (%) A 7 69,038 24 7,125 (10.3) 5,983 (84.0) 2,402 (40.1) 3,581 (59.9) B 5 15,362 45 1,013 (6.7) 768 (75.8) 185 (24.1) 583 (75.9) C 3 43,074 48 4,069 (9.5) 3,358 (82.5) 196 (5.8) 3,162 (94.2) D 13 198,011 45 22,473 (11.4) 19,589 (87.2) 3,519 (18.0) 16,070 (82.0) Total 28 325,485 34,680 (10.7) 29,698 (85.6) 6,302 (21.2) 23,396 (78.8)
BI-RADS, Breast Imaging Reporting and Data Systems; PROSPR, Population-based Research Optimizing Screening through Personalized Regimens.
Get Radiology Tree app to read full this article<
Table 2
Demographic Characteristics of Screening Mammograms
Patient Characteristics Screening Mammograms
n Abnormal Screening Results BI-RADS 0
n (%) Follow-up, ≤15 d
n (%) Age (y) 40–49 87,472 12,829 (14.7) 10,969 (85.5) 50–64 168,714 16,083 (9.9) 13,696 (85.2) 65–74 69,299 5,768 (8.3) 5,033 (87.3) Race and ethnicity White non-Hispanic 279,252 29,466 (10.5) 25,605 (86.9) Black non-Hispanic 23,345 2,531 (10.8) 1,895 (74.9) Hispanic 6,037 665 (11.0) 538 (80.9) Asian non-Hispanic 4,726 478 (10.1) 374 (78.2) Other non-Hispanic 6,561 808 (12.3) 668 (82.7) Missing 5,564 732 (13.2) 618 (84.4) Total 325,485 34,680 (10.7) 29,698 (85.6)
BI-RADS, Breast Imaging Reporting and Data Systems.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Communication of Mammography Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Association of Timely Follow-up and Facility-level Communication Modality
Communication Type Patient Misses Scheduled Appointment for Additional Imaging Facilities Endorsing in Survey (%) Follow-up in 1–15 d When Endorsed (%) vs Not Endorsed (%) Impact on Timely Follow-up After Adjustment \* ( P Value) OR (95% CI) To patient Phone 71.4 85.5 vs 72.8 .08 1.81 (0.93–3.53) Mail 32.1 85.1 vs 80.3 .0429 1.65 (1.02–2.69) Patient portal 3.6 81.8 vs 82.4 <.0001 2.05 (1.73–2.41) In person 0.0 — — — To provider Phone 28.6 89.3 vs 77.3 .0012 2.61 (1.46–4.66) Mail 17.9 76.9 vs 83.1 .63 1.30 (0.45–3.79) Electronic medical record 21.4 78.0 vs 83.3 .95 0.98 (0.49–1.93) Fax 7.1 82.2 vs 82.5 .57 0.79 (0.35–1.79)
CI, confidence interval; OR, odds ratio; PROSPR, Population-based Research Optimizing Screening through Personalized Regimens.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Bivariate Analysis
Get Radiology Tree app to read full this article<
Table 4
Association of Timely Follow-up and Facility-level Communication Modality
Communication Type Additional Imaging Recommended Facilities Endorsing in Survey
(%) Follow-up in 1–15 d When Endorsed (%) vs Not Endorsed (%) Impact on Timely Follow-up After Adjustment \* ( P Value) OR (95% CI) To patient Phone 89.3 83.5 vs 53.1 <.0001 4.63 (2.76–7.76) Mail 57.1 77.3 vs 87.8 .0012 0.47 (0.30–0.75) Patient portal 39.3 77.7 vs 85.4 .13 0.66 (0.39–1.12) In person 10.7 65.2 vs 82.7 .17 0.56 (0.25–1.27) To provider Phone 3.6 70.3 vs 82.5 .0051 1.24 (1.07–1.44) Mail 14.3 77.9 vs 83.5 .58 0.80 (0.36–1.76) Electronic medical record 82.1 81.9 vs 89.2 .0163 0.56 (0.35–0.90) Fax 42.9 81.3 vs 82.9 .65 0.85 (0.42–1.71)
CI, confidence interval; OR, odds ratio; PROSPR, Population-based Research Optimizing Screening through Personalized Regimens.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Multivariate Analysis
Get Radiology Tree app to read full this article<
Table 5
Association of Patient and Provider Communication Strategies with Timely Follow-up in Multivariate Analyses
Variable OR 95% CI_P_ Value Model A: Additional imaging recommended—patient communication \* Patient phone communication 3.63 2.29–5.76 <.0001 Patient mail communication 0.53 0.34–0.81 .003 Model B: Additional imaging recommended—provider communication \* Provider electronic medical recordcommunication 0.52 0.29–0.92 .02 Provider phone communication 0.64 0.36–1.16 .14 Model C: Patient misses scheduled appointment for additional imaging—patient communication \* Patient mail communication 1.65 1.01–2.69 .04 Patient portal communication 1.28 0.79–2.07 .32
CI, confidence interval; OR, odds ratio; PROSPR, Population-based Research Optimizing Screening through Personalized Regimens.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Sensitivity Analysis
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
Appendix
Supplementary Data
Get Radiology Tree app to read full this article<
Appendix S1
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Siu A.L., Force U.S.P.S.T.: Screening for breast cancer: U.S. preventive services task force recommendation statement. Ann Intern Med 2016; 164: pp. 279-296.
2. Zapka J.G., Taplin S.H., Solberg L.I., et. al.: A framework for improving the quality of cancer care: the case of breast and cervical cancer screening. Cancer Epidemiol Biomarkers Prev 2003; 12: pp. 4-13.
3. Beaber E.F., Kim J.J., Schapira M.M., et. al.: Unifying screening processes within the PROSPR consortium: a conceptual model for breast, cervical, and colorectal cancer screening. J Natl Cancer Inst 2015; 107: djv120
4. Onega T., Beaber E.F., Sprague B.L., et. al.: Breast cancer screening in an era of personalized regimens: a conceptual model and National Cancer Institute initiative for risk-based and preference-based approaches at a population level. Cancer 2014; 120: pp. 2955-2964.
5. Rudin R.S., Bates D.W.: Let the left hand know what the right is doing: a vision for care coordination and electronic health records. J Am Med Inf Assoc 2014; 21: pp. 13-16.
6. Tosteson A.N., Fryback D.G., Hammond C.S., et. al.: Consequences of false-positive screening mammograms. JAMA Intern Med 2014; 174: pp. 954-961.
7. Elmore J.G., Nakano C.Y., Linden H.M., et. al.: Racial inequities in the timing of breast cancer detection, diagnosis, and initiation of treatment. Med Care 2005; 43: pp. 141-148.
8. Wujcik D., Shyr Y., Li M., et. al.: Delay in diagnostic testing after abnormal mammography in low-income women. Oncol Nurs Forum 2009; 36: pp. 709-715.
9. Press R., Carrasquillo O., Sciacca R.R., et. al.: Racial/ethnic disparities in time to follow-up after an abnormal mammogram. J Womens Health 2008; 17: pp. 923-930.
10. Ashing-Giwa K.T., Gonzalez P., Lim J.W., et. al.: Diagnostic and therapeutic delays among a multiethnic sample of breast and cervical cancer survivors. Cancer 2010; 116: pp. 3195-3204.
11. Molina Y., Beresford S.A.A., Hayes Constant T., et. al.: Conversations about abnormal mammograms on distress and timely follow-up across ethnicity. J Cancer Educ 2017; 32: pp. 320-327.
12. Kerner J.F., Yedidia M., Padgett D., et. al.: Realizing the promise of breast cancer screening: clinical follow-up after abnormal screening among Black women. Prev Med 2003; 37: pp. 92-101.
13. Poon E.G., Haas J.S., Louise Puopolo A., et. al.: Communication factors in the follow-up of abnormal mammograms. J Gen Intern Med 2004; 19: pp. 316-323.
14. Marcus E.N., Koru-Sengul T., Miao F., et. al.: How do breast imaging centers communicate results to women with limited English proficiency and other barriers to care?. J Immigr Minor Health 2014; 16: pp. 401-408.
15. What constitutes an acceptable system for notifying patients of examination results. Available at https://www.fda.gov/Radiation-EmittingProducts/MammographyQualityStandardsActandProgram/Guidance/PolicyGuidanceHelpSystem/ucm135579.htm U.S. Department of Health and Human Services: U.S. Food & Drug Administration
16. Perry N., Broeders M., de Wolf C., et. al.: European guidelines for quality assurance in breast cancer screening and diagnosis. Fourth edition—summary document. Ann Oncol 2008; 19: pp. 614-622.
17. Ministry of Health : BreastScreen Aotearoa National Policy and Quality Standards. Wellington: Ministry of Health. Published in December 2013 (revised December 2016) by the Ministry of Health, PO Box 5013, Wellington 6145, New Zealand; ISBN 978-0-478-41584-12013.
18. Breast screening: Consolidated programme standards. PHE Publications gateway number: 2016720 PDF, 492KB. Updated 15 August 2017.
19. Report from the evaluation indicators working group. Guidelines for monitoring breast cancer screening program performance. Third Edition. Canadian partnership against cancer.2013.
20. BreastScreen Australia: A joint Australian State and Territory Government Program. Breastscreen Australia National Accreditation Handbook. March 2015. Endorsed by the Standard Committee on Screening 12 March 2015. Updated under the asupices of the BreastScreen Australia Accreditation Review Committee 21 September 2017.
21. Marcus E.N., Sanders L.M., Pereyra M., et. al.: Mammography result notification letters: are they easy to read and understand?. J Womens Health (Larchmt) 2011; 20: pp. 545-551.
22. Karliner L.S., Ma L., Hofmann M., et. al.: Language barriers, location of care, and delays in follow-up of abnormal mammograms. Med Care 2012; 50: pp. 171-178.
23. Allen J.D., Shelton R.C., Harden E., et. al.: Follow-up of abnormal screening mammograms among low-income ethnically diverse women: findings from a qualitative study. Patient Educ Couns 2008; 72: pp. 283-292.
24. Molina Y., Hohl S.D., Ko L.K., et. al.: Understanding the patient-provider communication needs and experiences of latina and non-latina white women following an abnormal mammogram. J Cancer Educ 2014; 29: pp. 781-789.
25. Marcus E.N., Drummond D., Dietz N.: Urban women’s preferences for learning of their mammogram result: a qualitative study. J Cancer Educ 2012; 27: pp. 156-164.
26. Poon E.G., Haas J.S., Puopolo A.L., et. al.: Communication factors in the follow-up of abnormal mammograms. J Gen Intern Med 2004; 19: pp. 316-323.
27. Perez-Stable E.J., Afable-Munsuz A., Kaplan C.P., et. al.: Factors influencing time to diagnosis after abnormal mammography in diverse women. J Womens Health (Larchmt) 2013; 22: pp. 159-166.
28. Wujcik D., Fair A.M.: Barriers to diagnostic resolution after abnormal mammography: a review of the literature. Cancer Nurs 2008; 31: pp. E16-E30.
29. Sasson J.P., Zand T., Lown B.A.: Communication in the diagnostic mammography suite: implications for practice and training. Acad Radiol 2008; 15: pp. 417-424.
30. Stewart K.A., Neumann P.J., Fletcher S.W., et. al.: The effect of immediate reading of screening mammograms on medical care utilization and costs after false-positive mammograms. Health Serv Res 2007; 42: pp. 1464-1482.
31. Burnside E.S., Park J.M., Fine J.P., et. al.: The use of batch reading to improve the performance of screening mammography. AJR Am J Roentgenol 2005; 185: pp. 790-796.
32. Ghate S.V., Soo M.S., Baker J.A., et. al.: Comparison of recall and cancer detection rates for immediate versus batch interpretation of screening mammograms. Radiology 2005; 235: pp. 31-35.
33. Carney P.A., Kettler M., Cook A.J., et. al.: An assessment of the likelihood, frequency, and content of verbal communication between radiologists and women receiving screening and diagnostic mammography. Acad Radiol 2009; 16: pp. 1056-1063.
34. Neuner J., Fedders M., Caravella M., et. al.: Meaningful use and the patient portal: patient enrollment, use, and satisfaction with patient portals at a later-adopting center. Am J Med Qual 2015; 30: pp. 105-113.
35. Ip I.K., Lacson R., Hentel K., et. al.: JOURNAL CLUB: predictors of provider response to clinical decision support: lessons learned from the Medicare imaging demonstration. AJR Am J Roentgenol 2017; 208: pp. 351-357.
36. Gregory M.E., Russo E., Singh H.: Electronic health record alert-related workload as a predictor of burnout in primary care providers. Appl Clin Inform 2017; 8: pp. 686-697.
37. Ancker J.S., Edwards A., Nosal S., et. al.: Effects of workload, work complexity, and repeated alerts on alert fatigue in a clinical decision support system. BMC Med Inform Decis Mak 2017; 17: pp. 36.
38. Singh H., Thomas E.J., Mani S., et. al.: Timely follow-up of abnormal diagnostic imaging test results in an outpatient setting are electronic medical records achieving their potential?. Arch Intern Med 2009; 169: pp. 1578-1586.
39. Rosenberg R.D., Haneuse S.J., Geller B.M., et. al.: Timeliness of follow-up after abnormal screening mammogram: variability of facilities. Radiology 2011; 261: pp. 404-413.
40. McCarthy A.M., Kim J.J., Beaber E.F., et. al.: Follow-up of abnormal breast and colorectal cancer screening by race/ethnicity. Am J Prev Med 2016; 51: pp. 507-512.
41. Anhang Price R., Zapka J., Edwards H., et. al.: Organizational factors and the cancer screening process. J Natl Cancer Inst Monogr 2010; 2010: pp. 38-57.