
Rationale and Objectives
The purpose of this evaluation was to compare the tagging quality of a barium-based regimen with that of iodine-based regimens for computed tomographic (CT) colonography.
Materials and Methods
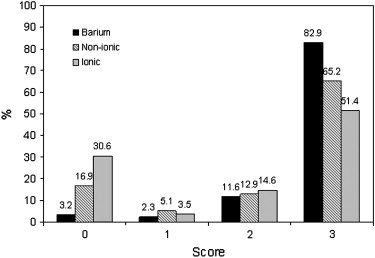
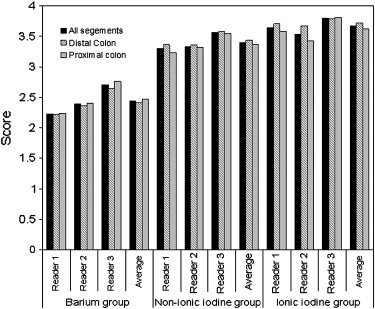
Tagging quality was assessed retrospectively in three different types of fecal-tagging CT colonographic cases: 24 barium-based cases, 22 nonionic iodine-based cases, and 24 ionic iodine-based cases. For the purpose of evaluation, the large intestine was divided into six segments, and the tagging homogeneity of a total of 420 segments (70 patients) was graded by three blinded readers from 0 (heterogeneous) to 4 (homogeneous).
Results
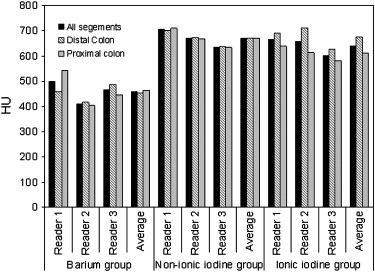
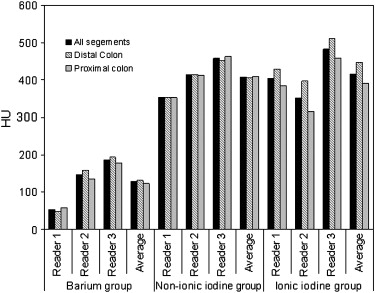
For barium-based cases, the average score for the three readers was 2.4, whereas it was 3.4 for nonionic iodine and 3.6 for ionic iodine. The percentages of segments that were assigned scores of 4 (excellent tagging [100%]) were 11.6%, 61.9%, and 72.9% for the barium-based, nonionic iodine-based, and ionic iodine-based regimens, respectively. The homogeneity scores of iodine-based fecal-tagging regimens were significantly higher than those of the barium-based fecal-tagging regimen ( P < .001). The CT attenuation values of tagging in the cases were also assessed: the minimum and maximum values were significantly higher for the iodine-based regimens than for the barium-based regimen ( P < .001).
Conclusions
The iodine-based fecal-tagging regimens provide significantly greater homogeneity in oral-tagging fecal material than the barium-based fecal-tagging regimen. Iodine-based fecal-tagging regimens can provide an appropriate method for use in nonlaxative or minimum-laxative CT colonography.
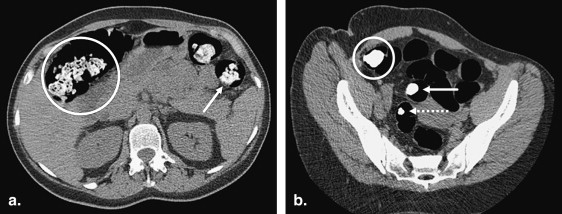
Thorough bowel cleansing and adequate distension are necessary for successful computed tomographic (CT) colonographic (CTC) examinations. However, patients often perceive these two procedures as the most unpleasant aspects of CTC examinations . Fecal tagging by orally administered positive-contrast agents can be used for the effective differentiation of fecal material from polyps by enhancing residual stool and fluid, thus increasing the specificity of polyps . For distinguishing tagged fecal contents reliably from soft tissue lesions in the large intestine, the tagging of fecal material should be homogeneous . In general, three contrast agents are suitable for fecal-tagging CT colonography: barium sulfate, ionic iodine, and nonionic iodine . However, to our knowledge, the quality of tagging using these three contrast agents has never been compared in fecal-tagging CT colonography.
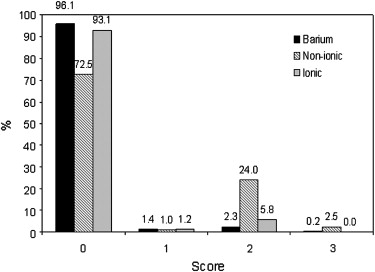
In this study, we retrospectively compared the quality of tagging using three contrast agents with either nonlaxative or minimum-laxative regimens. The quality of tagging was assessed in terms of homogeneity and CT attenuation values (in Hounsfield units [HU]) of the residual fecal material. We also evaluated the observed presence of residual stool and fluid for each regimen.
Materials and methods
Study Group
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Fecal-Tagging Regimens
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
CT Colonography
Get Radiology Tree app to read full this article<
Evaluation of Residual Stool and Fluid and Tagging Quality
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Bowel Preparation
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Tagging Quality
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Pickhardt P.J.: Screening CT colonography: how I do it. AJR Am J Roentgenol 2007; 189: pp. 290-298.
2. Gluecker T.M., Johnson C.D., Harmsen W.S., et. al.: Colorectal cancer screening with CT colonography, colonoscopy, and double-contrast barium enema examination: prospective assessment of patient perceptions and preferences. Radiology 2003; 227: pp. 378-384.
3. Ristvedt S.L., McFarland E.G., Weinstock L.B., Thyssen E.P.: Patient preferences for CT colonography, conventional colonoscopy, and bowel preparation. Am J Gastroenterol 2003; 98: pp. 578-585.
4. Callstrom M.R., Johnson C.D., Fletcher J.G., et. al.: CT colonography without cathartic preparation: feasibility study. Radiology 2001; 219: pp. 693-698.
5. Lefere P.A., Gryspeerdt S.S., Dewyspelaere J., Baekelandt M., Van Holsbeeck B.G.: Dietary fecal tagging as a cleansing method before CT colonography: initial results polyp detection and patient acceptance. Radiology 2002; 224: pp. 393-403.
6. Bielen D., Thomeer M., Vanbeckevoort D., et. al.: Dry preparation for virtual CT colonography with fecal tagging using water-soluble contrast medium: initial results. Eur Radiol 2003; 13: pp. 453-458.
7. Thomeer M., Carbone I., Bosmans H., et. al.: Stool tagging applied in thin-slice multidetector computed tomography colonography. J Comput Assist Tomogr 2003; 27: pp. 132-139.
8. Iannaccone R., Laghi A., Catalano C., et. al.: Computed tomographic colonography without cathartic preparation for the detection of colorectal polyps. Gastroenterology 2004; 127: pp. 1300-1311.
9. Gryspeerdt S., Lefere P., Herman M., et. al.: CT colonography with fecal tagging after incomplete colonoscopy. Eur Radiol 2005; 15: pp. 1192-1202.
10. Barish M.A., Soto J.A., Ferrucci J.T.: Consensus on current clinical practice of virtual colonoscopy. AJR Am J Roentgenol 2005; 184: pp. 786-792.
11. Zalis M.E., Perumpillichira J.J., Magee C., Kohlberg G., Hahn P.F.: Tagging-based, electronically cleansed CT colonography: evaluation of patient comfort and image readability. Radiology 2006; 239: pp. 149-159.
12. Kim D.H., Pickhardt P.J., Hinshaw J.L., Taylor A.J., Mukherjee R., Pfau P.R.: Prospective blinded trial comparing 45-mL and 90-mL doses of oral sodium phosphate for bowel preparation before computed tomographic colonography. J Comput Assist Tomogr 2007; 31: pp. 53-58.
13. Jensch S., de Vries A.H., Pot D., et. al.: Image quality and patient acceptance of four regimens with different amounts of mild laxatives for CT colonography. AJR Am J Roentgenol 2008; 191: pp. 158-167.
14. Lefere P., Gryspeerdt S., Marrannes J., Baekelandt M., Van Holsbeeck B.: CT colonography after fecal tagging with a reduced cathartic cleansing and a reduced volume of barium. AJR Am J Roentgenol 2005; 184: pp. 1836-1842.
15. Nagata K., Endo S., Ichikawa T., et. al.: Polyethylene glycol solution (PEG) plus contrast medium vs PEG alone preparation for CT colonography and conventional colonoscopy in preoperative colorectal cancer staging. Int J Colorectal Dis 2007; 22: pp. 69-76.
16. Sugiyama A., Ohashi Y., Gomi A., et. al.: Colorectal screening with single scan CT colonography in children. Pediatr Surg Int 2007; 23: pp. 987-990.
17. Taylor S.A., Slater A., Burling D.N., et. al.: CT colonography: optimisation, diagnostic performance and patient acceptability of reduced-laxative regimens using barium-based faecal tagging. Eur Radiol 2008; 18: pp. 32-42.
18. Johnson C.D., Manduca A., Fletcher J.G., et. al.: Noncathartic CT colonography with stool tagging: performance with and without electronic stool subtraction. AJR Am J Roentgenol 2008; 190: pp. 361-366.
19. Summers R.M., Handwerker L.R., Pickhardt P.J., et. al.: Performance of a previously validated CT colonography computer-aided detection system in a new patient population. AJR Am J Roentgenol 2008; 191: pp. 168-174.
20. Neri E, Turini F, Cerri F, Vagli P, Bartolozzi C. CT colonography: same-day tagging regimen with iodixanol and reduced cathartic preparation. Abdom Imaging. In press.
21. Nagata K., Okawa T., Honma A., Endo S., Kudo S., Yoshida H.: Full-laxative vs. minimum-laxative fecal-tagging CT colonography using 64-detector-row CT: prospective blinded comparison of diagnostic performance, tagging quality, and patient acceptance. Acad Radiol 2009; 16: pp. 780-789.
22. Ross B.: Fundamentals of biostatistics.1995.Duxbury PressNew York
23. Taylor S.A., Laghi A., Lefere P., Halligan S., Stoker J.: European Society of Gastrointestinal and Abdominal Radiology (ESGAR): consensus statement on CT colonography. Eur Radiol 2007; 17: pp. 575-579.
24. Nagata K., Näppi J., Cai W., Yoshida H.: Minimum-invasive early diagnosis of colorectal cancer with CT colonography: techniques and clinical value. Expert Opin Med Diagn 2008; 2: pp. 1233-1246.
25. Johnson K.T., Carston M.J., Wentz R.J., Manduca A., Anderson S.M., Johnson C.D.: Development of a cathartic-free colorectal cancer screening test using virtual colonoscopy: a feasibility study. AJR Am J Roentgenol 2007; 188: pp. W29-W36.
26. Langer R., Kaufmann H.J.: Nonionic contrast media for gastro-intestinal studies in newborns and infants. J Belge Radiol 1987; 70: pp. 211-216.
27. Horton K.M., Fishman E.K., Gayler B.: The use of iohexol as oral contrast for computed tomography of the abdomen and pelvis. J Comput Assist Tomogr 2008; 32: pp. 207-209.
28. American College of Radiology. Manual on contrast media: version 6: 2008. Available at: http://www.scribd.com/doc/2952016/Contrast-Media-Administration-Guidelines-by-the-ACR-American-College-of-Radiology-Version-6-2008 . Accessed February 9, 2009.
29. Laerum F., Stordahl A., Solheim K.E., Haugstvedt J.R., Roald H.E., Skinningsrud K.: Intestinal follow-through examinations with iohexol and iopentol. Permeability alterations and efficacy in patients with small bowel obstruction. Invest Radiol 1991; 26: pp. S177-S181.
30. Lonnemark M., Magnusson A.: Oral contrast media in CT of the abdomen. Iohexol of different concentrations as a gastrointestinal contrast medium. Acta Radiol 1995; 36: pp. 396-398.
31. Stordahl A., Laerum F., Gjolberg T., Enge I.: Water-soluble contrast media in radiography of small bowel obstruction. Comparison of ionic and non-ionic contrast media. Acta Radiol 1988; 29: pp. 53-56.
32. Cohen M.D., Towbin R., Baker S., et. al.: Comparison of iohexol with barium in gastrointestinal studies of infants and children. AJR Am J Roentgenol 1991; 156: pp. 345-350.
33. Diederichs G., Franiel T., Asbach P., Romano V., Hamm B., Rogalla P.: Oral administration of intravenous contrast media: a tasty alternative to conventional oral contrast media in computed tomography. Rofo 2007; 179: pp. 1061-1067.
34. Dachman A.H., Dawson D.O., Lefere P., et. al.: Comparison of routine and unprepped CT colonography augmented by low fiber diet and stool tagging: a pilot study. Abdom Imaging 2007; 32: pp. 96-104.
35. Kalra M.K., Maher M.M., Toth T.L., et. al.: Techniques and applications of automatic tube current modulation for CT. Radiology 2004; 233: pp. 649-657.