
Rationale and Objectives
To compare the effectiveness of chest dual-energy subtraction digital tomosynthesis (DES-DT) imaging with that of DES radiography for detecting simulated pulmonary nodules with and without calcifications.
Materials and Methods
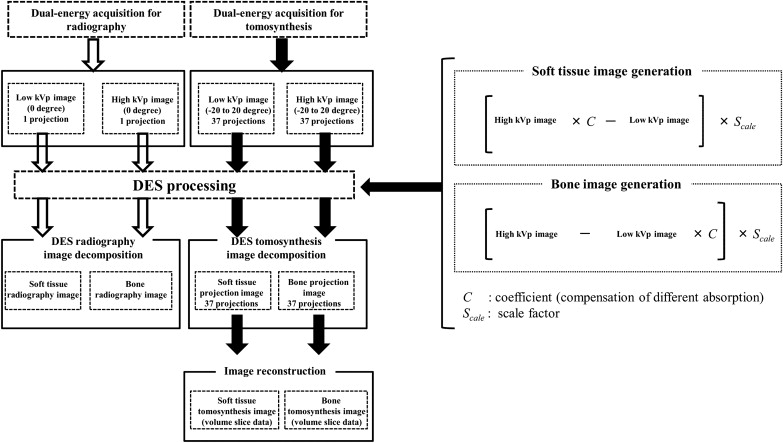
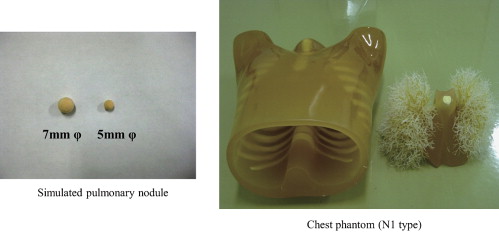
A DES-DT and DES radiography system (SonialVision Safire II, Shimadzu Co, Kyoto, Japan) with pulsed x-rays and rapid kV switching was used to detect simulated pulmonary nodules (5 and 7 mm φ , ground-glass opacity). Low-voltage (60 kVp), high-voltage (120 kVp), and soft-tissue or bone-subtracted tomograms of the desired layer thicknesses were reconstructed from the image data acquired during a single tomographic scan using a three-dimensional filtered back-projection algorithm, bone- and soft tissue‑subtracted images, and a scan angle of 40°. In the analysis, we considered the signal-to-noise ratio (SNR) computed for various sizes and degree of calcification of the simulated pulmonary nodules. We examined 30 samples with and 30 samples without different degrees of simulated pulmonary nodules by both DES radiography and DES-DT imaging. Based on the evaluations of five thoracic radiologists, receiver operating characteristic curves were compared to assess the detection accuracy of the two methods.
Results
SNR and quality of images obtained by DES-DT imaging were significantly superior to those obtained by DES radiography. Based on the results of the ROC analysis, the detection accuracy of DES-DT was significantly greater than that of DES radiography (7 mm φ without calcification P < .03; with calcification P < .003).
Conclusion
DES-DT imaging exhibited greater sensitivity than DES radiography for detecting simulated nodules, especially large nodules, with and without calcifications.
Lung cancer is currently the leading cause of cancer death and continues to be an increasing cause of death worldwide. Because of its high sensitivity, normal-dose helical computed tomography (CT) is currently considered the gold standard for lung cancer detection. Previous studies have indicated that low-dose helical CT can detect early-stage lung cancer and thus lead to decreased morbidity . CT is advantageous because it is not susceptible to the problem of reduced accuracy caused by overlapping anatomy. However, it has disadvantages such as high radiation dose and cost compared to chest radiography. In contrast, the advantages of chest radiography include short examination time, low cost, and easy access; however, low sensitivity and specificity are important disadvantages. In chest radiography, the three-dimensional chest is projected onto a two-dimensional image, and, therefore, for many analyses, the capability to detect pathological findings is limited by overlapping anatomy rather than quantum noise. Chest radiography has been shown to have relatively low sensitivity for detecting pulmonary nodules. This poor sensitivity precludes its use as a screening method, despite its low cost, low dose, and widespread availability of radiographic devices.
Two radiographic findings indicate a benign lesion when differentiating between benign and malignant pulmonary masses: the presence of calcifications in the mass and mass stability . A benign pattern of the calcifications has been considered necessary to exclude malignancy . For evaluating diffusely disseminated pulmonary nodules, identification of calcifications in the nodules has been helpful in limiting differential diagnosis . Conventional radiography and tomography have been used to detect calcifications, but they have been largely replaced by CT . However, CT has several inherent problems, including motion artifacts and variation in reconstruction algorithms used by different scanners. Despite recent developments in CT techniques, difficulties such as shifting of the slice level in thin-section CT images acquired during different breaths as well as clarifying the characteristics and distribution of calcifications relative to soft-tissue components of the mass have persisted.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
DES-DT and DES Radiography System
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Phantom Specification and Simulated Pulmonary Nodules
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Evaluation of Signal-to-noise Ratio
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Observer Study
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
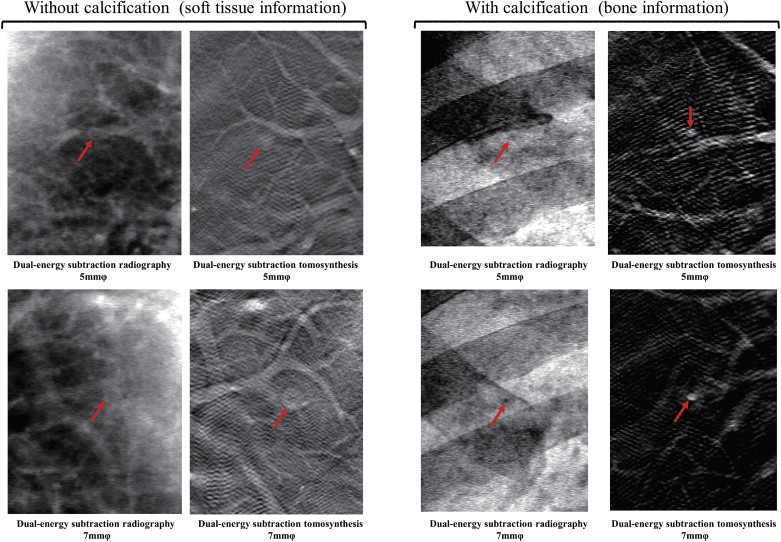
Table 1
Relationship between Average SNR and Simulated Pulmonary Nodule Size as well as with and without Calcifications
Without Calcifications With Calcifications Average SNR (DES Radiography) Average SNR (DES-DT) Average SNR (DES Radiography) Average SNR (DES-DT) 5 mm-φ 2.29 3.02 0.25 1.24 7 mm-φ 0.05 1.89 1.55 2.32
DES, dual-energy subtraction; DT, digital tomosynthesis; SNR, signal-to-noise ratio.
In processing by dual-energy subtraction tomosynthesis imaging, the results confirm that the SNR value increases when viewing a large nodule in the presence of calcifications.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Comparison of the Area under the Curve for the Detection Accuracy of Dual-energy Subtraction Tomosynthesis Imaging and Dual-energy Subtraction Radiography by the Observers
Without Calcifications (5 mm-φ) Without Calcifications (7 mm-φ) With Calcifications DES-DT DES-R DES-DT DES-R DES-DT DES-R Observer 1 0.884 0.832 0.903 0.870 0.934 0.685 Observer 2 0.668 0.500 0.958 0.500 0.904 0.500 Observer 3 0.784 0.608 0.906 0.500 0.932 0.836 Observer 4 0.590 0.676 0.837 0.695 0.884 0.543 Observer 5 0.647 0.711 0.844 0.669 0.836 0.627 Mean 0.707 0.665 0.890 0.647 0.989 0.638 Difference 95% CI (0.041 to 0.2400) (0.243 to 0.4690) (0.259 to 0.4143) Significant Not significant Significant ( P < .03) Significant ( P < .003)
CI, confidence interval; DES, dual-energy subtraction; DT, digital tomosynthesis; R, radiography.
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Yankelevitz D.F., Reeves A.P., Kostis W.J., et. al.: Small pulmonary nodules: volumetrically determined growth rates based on CT evaluation. Radiology 2000; 217: pp. 251-256.
2. Godwin J.D.: The solitary pulmonary nodule. Radiol Clin North Am 1983; 21: pp. 709-721.
3. Littleton J.T.: Pluridirectional tomography in diagnosis and management of early bronchogenic carcinoma.Little M.L.Sectional imaging methods. A comparison.1983.University Park PressBaltimore, MD:pp. 155-173.
4. Siegelman S.S., Khouri N.F., Leo F.P., et. al.: Solitary pulmonary nodules. CT assessment. Radiology 1986; 160: pp. 307-312.
5. Siegelman S.S., Zerhouni E.A., Loe F.P., et. al.: CT of the solitary pulmonary nodule. AJR Am J Roentgenol 1980; 135: pp. 1-13.
6. Zerhouni E.A., Caskey C., Khouri N.F.: The pulmonary nodules. Semin Ultrasound CT MR 1988; 9: pp. 67-78.
7. Fraser R.G., Hickey N.M., Niklason L.T., et. al.: Calcification in pulmonary nodules. Detection with dual-energy digital radiography. Radiology 1986; 160: pp. 595-601.
8. McLendon R.E., Roggli V.L., Foster W.L., et. al.: Carcinoma of the lung with osseous stromal metaplasia. Arch Pathol Lab Med 1985; 109: pp. 1051-1053.
9. O’Keefe M.E., Good C.A., McNonald J.R.: Calcification in solitary nodules of the lung. AJR Am J Roentgenol 1957; 77: pp. 1023-1033.
10. Siegelman S.S., Zerhouni E.A.: Computed tomography of the solitary pulmonary nodule. In: Sectional imaging methods.Little M.L.Sectional imaging methods. A comparison.1983.University Park PressBaltimore, MD:pp. 175-182.
11. Burgener F.A., Kormano M.: Differential diagnosis in conventional radiology.1991.Thieme VerlagBerlin, Germany
12. Brody W.R., Butt G., Hall A., Macovski A.: A method for selective tissue and bone visualization using dual-energy scanned projection radiography. Med Phys 1981; 8: pp. 659-667.
13. Hickey N.M., Niklason L.T., Sabbagh E., et. al.: Dual-energy digital radiographic quantification of calcium in simulated pulmonary nodules. AJR Am J Roentgenol 1987; 148: pp. 19-24.
14. Ishigaki T., Sakuma S., Horikawa Y., et. al.: One-shot dual-energy subtraction imaging. Radiology 1986; 161: pp. 271-273.
15. Ishigaki T., Sakuma S., Ikeda M.: One-shot dual-energy subtraction chest imaging with computed radiography. Radiology 1988; 168: pp. 67-72.
16. Nishitani H., Umezu Y., Ogawa K., et. al.: Dual-energy projection radiography using condenser X-ray generator and digital radiography apparatus. Radiology 1986; 161: pp. 533-535.
17. Dobbins J.T., Godfrey D.J.: Digital x-ray tomosynthesis: current state of the art and clinical potential. Phys Med Biol 2003; 48: pp. R65-R106.
18. Gomi T., Hirano H.: Clinical potential of digital linear tomosynthesis imaging of total joint arthroplasty. J Digit Imaging 2008; 21: pp. 312-322.
19. Berbaum K. DBM MRMC software 2.2. Available at: http://perception.radiology.uiowa.edu . Accessed January 7, 2009.
20. Hanley J.A., McNeil B.J.: The meaning and use of the area under receiver operating characteristic (ROC) curves. Radiology 1982; 143: pp. 29-36.
21. Hanley J.A., McNeil B.J.: A method of comparing the areas under receiver operating characteristic curves derived from the same cases. Radiology 1983; 148: pp. 839-843.