
Rationale and Objectives
Invasive coronary angiography (ICA) with fractional flow reserve (FFR) assessment is the reference standard for the detection of hemodynamically relevant coronary lesions. We have investigated whether coronary computed tomography angiography (cCTA)-derived FFR (fractional flow reserve from coronary computed tomographic angiography [CT-FFR]) measurement improves diagnostic accuracy over cCTA.
Methods and Results
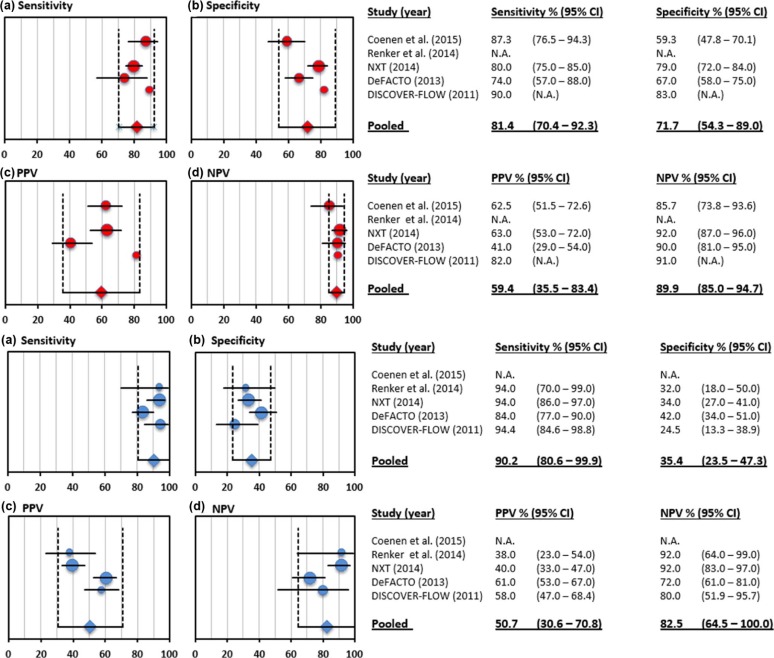
A literature search was performed for studies comparing invasive FFR, cCTA, and CT-FFR. The analysis included three prospective multicenter trials and two retrospective single-center studies; a total of 765 patients and 1306 vessels were included in the meta-analysis. Compared to invasive FFR on a per-lesion basis, CT-FFR reached a pooled sensitivity, specificity, positive predictive value, and negative predictive value of 83.7% (95% confidence interval [CI]: 78.1–89.3), 74.7% (95% CI: 52.2–97.1), 64.8% (95% CI: 52.1–77.5), and 90.1% (95% CI: 80.8–99.3) compared to 84.6% (95% CI: 78.1–91.1), 49.7% (95% CI: 31.1–68.4), 39.0% (95% CI: 28.0–50.1), and 87.3% (95% CI: 72.5–100.0) for cCTA alone. In 634 vessels with intermediate stenosis (30%–70%), sensitivity, specificity, positive predictive value, and negative predictive value were 81.4% (95% CI: 70.4–92.9), 71.7% (95% CI: 54.5–89.0), 59.4% (95% CI: 35.5–83.4), and 89.9% (95% CI: 85.0–94.7) compared to 90.2% (95% CI: 80.6–99.9), 35.4% (95% CI: 23.5–47.3), 50.7% (95% CI: 30.6–70.8), and 82.5% (95% CI: 64.5–100.0) for cCTA alone. The summary area under the receiver operating characteristic curve of CT-FFR was superior to cCTA alone on a per-vessel (0.90 [95% CI: 0.82–0.98] vs 0.74 [95% CI: 0.63–0.86]; P = .0047) and for intermediate stenoses (0.76 [95% CI: 0.65–0.88] vs 0.57 [95% CI: 0.49–0.66]; P = .0027).
Conclusion
CT-FFR significantly improves specificity without noticeably altering the sensitivity of cCTA with invasive FFR as a reference standard for the detection of hemodynamically relevant stenosis.
Introduction
Coronary computed tomography angiography (cCTA) is an established noninvasive method for the exclusion of obstructive coronary artery disease (CAD) in low to intermediate risk patient populations . Although it tends to overestimate lesion severity compared to invasive coronary angiography (ICA), cCTA allows for the noninvasive assessment of coronary artery anatomy. However, the hemodynamic significance of coronary stenoses cannot be sufficiently evaluated with cCTA alone . Fractional flow reserve (FFR) is an invasive technique performed during cardiac catheterization that evaluates the functional significance of indeterminate coronary stenoses and provides guidance for lesion-specific revascularization therapy .
At this time, three large prospective clinical trials have demonstrated the diagnostic value of a noninvasive FFR (fractional flow reserve from coronary computed tomographic angiography [CT-FFR]) algorithm (HeartFlow, Inc., Redwood City, CA) based on fluid-dynamic modeling of coronary flow using diagnostic cCTA data acquired at rest . Furthermore, an initial study presented results on the diagnostic performance of an alternative on-site algorithm (Siemens Healthcare, Forchheim, Germany), also based on fluid-dynamic modeling; these results were subsequently corroborated by a larger study . Taken together, these investigations have demonstrated that algorithm-based noninvasive FFR derivation from cCTA compares favorably to the diagnostic gold standard of invasive FFR.
Methods
Study Design and Search Criteria
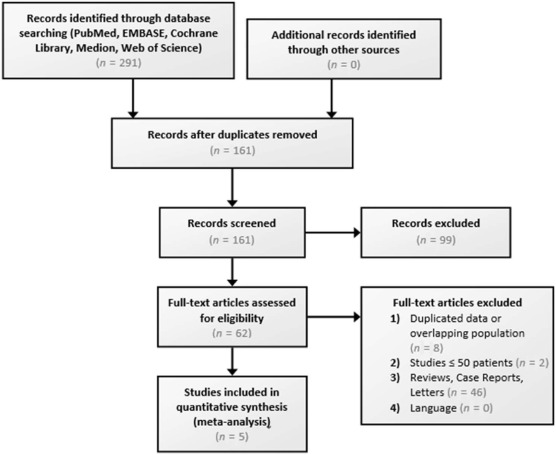
The present study was conducted in compliance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses statement to establish standards to ensure the quality of meta-analyses . We performed a literature search on the Science Citation Index, EMBASE, Cochrane Library, Google Scholar, and PubMed databases until June 2015 using the following keywords: CT-based FFR, FFR CT, noninvasive FFR, noninvasive fractional flow reserve, non-invasive FFR, and non-invasive fractional flow reserve. Studies meeting the following inclusion criteria comprised the final meta-analysis: study design involving diagnostic accuracy assessment, age of all study subjects ≥18 years, subject presentation with suspected or known CAD, CT-FFR as the index test, invasive FFR as the diagnostic reference standard, CT-FFR and invasive FFR in at least 50 patients. Duplicate studies were excluded. The study selection process is diagrammed in Figure 1 .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Study Population
Get Radiology Tree app to read full this article<
cCTA Protocol and Assessment
Get Radiology Tree app to read full this article<
ICA with FFR Measurement
Get Radiology Tree app to read full this article<
CT-FFR Computation
Get Radiology Tree app to read full this article<
Statistical Analyses
Get Radiology Tree app to read full this article<
Results
Patient Characteristics
Get Radiology Tree app to read full this article<
TABLE 1
Study Design and Baseline Characteristics Presented as Mean ± Standard Deviation or Frequency (%)
Koo et al.
(DISCOVER-FLOW) Min et al.
(DeFACTO) Nørgaard et al.
(NXT Trial) Renker et al. Coenen et al. Journal J Am Coll Cardiol JAMA J Am Coll Cardiol Am J Cardiol Radiology Year 2011 2012 2014 2014 2014 Study design Multicenter,
(4 centers
in 3 countries),
prospective Multicenter
(17 centers
in 5 countries),
prospective Multicenter
(10 centers
in 8 countries),
prospective Single-center,
retrospective Single-center,
retrospective CT system 64- or 256-detector CT 64- or higher detector CT 64- or higher detector CT 64- or 128-section dual-source CT 64- or 128-section dual-source CT CT-FFR software
(manufacturer) FFR CT (HeartFlow, Inc., Redwood City, CA),
V1.2 FFR CT (HeartFlow, Inc., Redwood City, CA),
V1.2 FFR CT (HeartFlow, Inc., Redwood City, CA),
V1.4 cFFR (Siemens Healthcare, Forchheim, Germany),
V1.4 + cFFR (Siemens Healthcare, Forchheim, Germany),
V1.4 + Number of included patients 103 252 251 53 106 Number of excluded patients NA 33/285 (11.6%) 111/365 (30.4%) 19/64 (29.7%) 16/122 (13.1%) Number of vessels 159 407 484 67 189 Age (years) 62.7 ± 8.5 62.9 ± 8.7 64 ± 10 61.2 ± 12.0 61.4 ± 9.2 Male (%) 74 (72%) 178 (70.6%) 162 (64%) 34 (64%) 82 (77%) BMI (kg/m 2 ) 25.8 ± 3.5 NA 26 ± 3 28.9 ± 6.5 27.2 ± 4.0 Diabetes mellitus (%) 26 (26%) 53 (21.2%) 58 (23%) 18 (32%) 20 (19%) Hypertension (%) 67 (65%) 179 (71.2%) 174 (69%) 31 (54%) 63 (59%) Hyperlipidemia (%) 67 (65%) 201 (79.8%) 200 (79%) 21 (54%) 63 (59%) Current smoker (%) 24 (36%) 44 (17.5%) 46 (18%) 8 (14%) 26 (25%)
BMI, body mass index; CT, computed tomography; CT-FFR, fractional flow reserve from coronary computed tomographic angiography; DeFACTO, Determination of Fractional Flow Reserve by Anatomic Computed Tomographic Angiography; DISCOVER-FLOW, Diagnosis of Ischemia-Causing Stenoses Obtained via Noninvasive Fractional Flow Reserve; FFR, fractional flow reserve; NA, not available; NXT, Analysis of Coronary Blood Flow Using CT Angiography, Next Steps.
TABLE 2
Vessel Characteristics According to cCTA, ICA, FFR, and CT-FFR
Koo et al.
(DISCOVER-FLOW) Min et al.
(DeFACTO) Nørgaard et al.
(NXT Trial) Renker et al. Coenen et al. Invasive coronary angiography (ICA) ICA stenosis ≥50% (%) NA 190(46.5%) 81(32%) 44(66%) 87(46.0%) FFR ≤0.80 (%) 35 (23%) 151(37.1%) 100(21%) 20(30%) 80(42.3%) Coronary computed tomography angiography (cCTA) Agatston score (±SD) NA 381.5 ± 401.0 302 ± 468 778.4 ± 731.1 555 ± 542 cCTA stenosis ≥50% (%) NA 216(53.2%) 220(87%) 55(82%) 133(70.4%) CT-FFR ≤0.80 (%) NA 216(53.3%) 135(28%) 24(36%) 108(57.1%)
CT-FFR, fractional flow reserve from coronary computed tomographic angiography; DeFACTO, Determination of Fractional Flow Reserve by Anatomic Computed Tomographic Angiography; DISCOVER-FLOW, Diagnosis of Ischemia-Causing Stenoses Obtained via Noninvasive Fractional Flow Reserve; FFR, fractional flow reserve; NA, not available; NXT, Analysis of Coronary Blood Flow Using CT Angiography, Next Steps; SD, standard deviation.
Get Radiology Tree app to read full this article<
Diagnostic Accuracy of CT-FFR and cCTA for Diagnosing Ischemia
Get Radiology Tree app to read full this article<
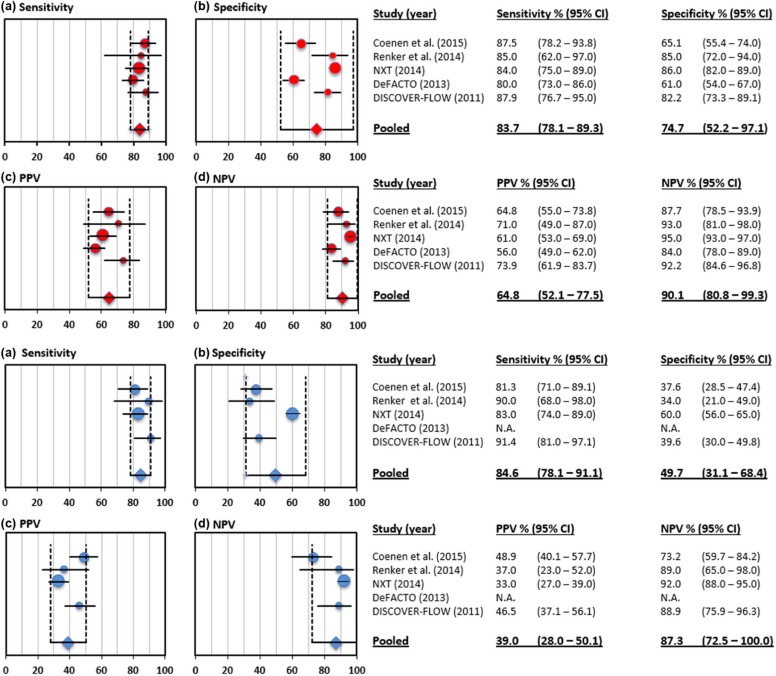
TABLE 3
Diagnostic Accuracy of CT-FFR and cCTA Compared to Invasive FFR as the Reference Standard on a Per-Vessel Level
Koo et al.
(DISCOVER-FLOW) Min et al.
(DeFACTO) Nørgaard et al.
(NXT Trial) Renker et al. Coenen et al. Pooled Per-vessel ( n = 1306) diagnostic performance of CT-FFR <0.80 (95% CI) and cCTA ≥50% (95% CI) [in brackets] Number of vessels 159 407 484 67 189 1306 Sensitivity (%) 87.9 (76.7–95.0)
[91.4 (81.0–97.1)] 80 (73–86)
[NA] 84 (75–89)
[83 (74–89)] 85 (62–97)
[90 (68–98)] 87.5 (78.2–93.8)
[81.3 (71.0–89.1)] 83.7 (78.1–89.3)
[84.6 (78.1–91.1)] Specificity (%) 82.2 (73.3–89.1)
[39.6 (30.0–49.8)] 61 (54–67)
[NA] 86 (82–89)
[60 (56–65)] 85 (72–94)
[34 (21–49)] 65.1 (55.4–74.0]
[37.6 (28.5–47.4)] 74.7 (52.2–97.1)
[49.7 (31.1–68.4)] PPV (%) 73.9 (61.9–83.7)
[46.5 (37.1–56.1)] 56 (49–62)
[NA] 61 (53–69)
[33 (27–39)] 71 (49–87)
[37 (23–52)] 64.8 (55.0–73.8)]
[48.9 (40.1–57.7)] 64.8 (52.1–77.5)
[39.0 (28.0–50.1)] NPV (%) 92.2 (84.6–96.8]
[88.9 (75.9–96.3)] 84 (78–89)
[NA] 95 (93–97)
[92 (88–95)] 93 (81–98)
[89 (65–98)] 87.7 (78.5–93.9)
[73.2 (59.7–84.2)] 90.1 (80.8–99.3)
[87.3 (72.5–100.0)] Accuracy (%) 84.3 (77.7–90.0)
[58.5 (50.4–66.2)] NA
[NA] 86 (83–89)
[65 (61–69)] NA
[NA] 74.6 (68.4–80.8)
[56.1 (49.0–63.2)] 83.1 (74.0–92.2)
[61.7 (56.6–66.9)] AUC 0.90 (NA)
[0.75 (NA)]
( P = .001) NA
[NA] 0.93 (0.91–0.95)
[0.79 (0.74–0.84)]
( P < .001) 0.92 (NA)
[0.72(NA)]
( P < .005) 0.83 (NA)
[0.64 (NA)]
( P < .001) 0.90 (0.82−0.98)
[0.74 (0.63–0.86)]
( P = .0047) Correlation between CT-FFR and FFR Per-vessel correlation Pearson’s
correlation coefficient =
0.678 (p < 0.0001) Pearson
correlation coefficient = 0.63
( P = NA) Pearson
correlation coefficient = 0.82
( P < .001) NA Pearson
correlation coefficient = 0.59
( P = NA) NA Spearman’s rank
correlation coefficient =
0.717 (p < 0.0001) NA NA Spearman rank
correlation coefficient = 0.66
( P < .001) NA NA
AUC, area under the receiver operating characteristic curve; cCTA, coronary computed tomographic angiography; CI, confidence interval; CT-FFR, fractional flow reserve from coronary computed tomographic angiography; DeFACTO, Determination of Fractional Flow Reserve by Anatomic Computed Tomographic Angiography; DISCOVER-FLOW, Diagnosis of Ischemia-Causing Stenoses Obtained via Noninvasive Fractional Flow Reserve; FFR, fractional flow reserve; NA, not available; NPV, negative predictive value; NXT, Analysis of Coronary Blood Flow Using CT Angiography, Next Steps; PPV, positive predictive value.
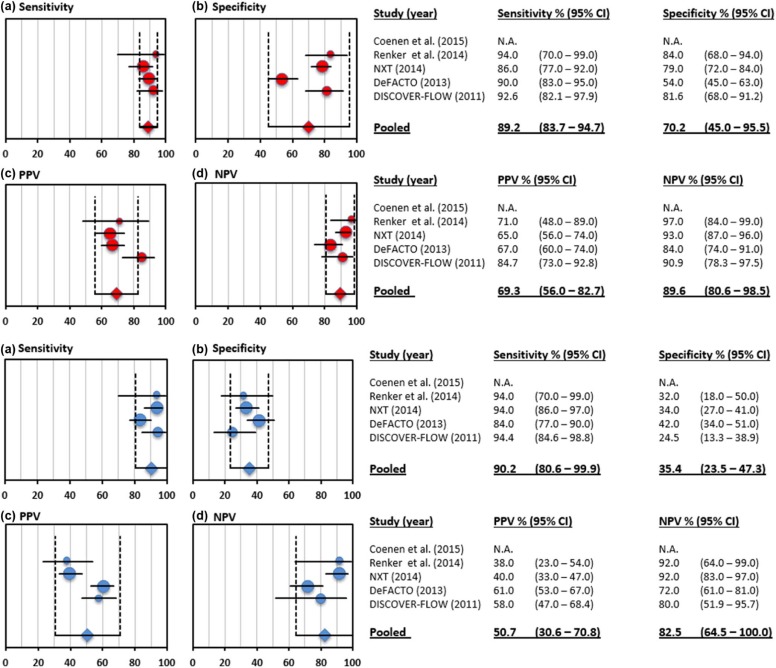
TABLE 4
Diagnostic Accuracy of CT-FFR and cCTA Compared to Invasive FFR as the Reference Standard on a Per-Patient Level
Per-Patient ( n = 765) Diagnostic Performance of CT-FFR <0.80 (95% CI) and cCTA ≥50% (95% CI) [in brackets] Number of included patients 103 252 251 53 106 765 Sensitivity (%) 92.6 (82.1–97.9)
[94.4 (84.6–98.8)] 90 (83–95)
[84 (77–90)] 86 (77–92)
[94 (86–97)] 94 (70–99)
[94 (70–99)] NA
[NA] 89.2 (83.7–94.7)
[90.2 (80.6–99.9)] Specificity (%) 81.6 (68.0–91.2)
[24.5 (13.3–38.9)] 54 (45–63)
[42 (34–51)] 79 (72–84]
[34 (27–41)] 84 (68–94)
[32 (18–50)] NA
[NA] 70.2 (45.0–95.5)
[(35.4 (23.5–47.3)] PPV (%) 84.7 (73.0–92.8)
[58.0 (47.0–68.4)] 67 (60–74)
[61 (53–67)] 65 (56–74)
[40 (33–47)] 71 (48–89)
[38 (23–54)] NA
[NA] 69.3 (56.0–82.7)
[50.7 (30.6–70.8)] NPV (%) 90.9 (78.3–97.5)
[80.0 (51.9–95.7)] 84 (0.74–0.91)
[72 (61–81)] 93 (87–96]
[92 (83–97)] 97 (84–99)
[92 (64–99)] NA
[NA] 89.6 (80.6–98.5)
[82.5 (64.4–100.0)] Accuracy (%) 87.4 (79.4–93.1)
[61.2 (51.1–70.6)] NA
[NA] 81 (76–85)
[53 (47–57)] NA
[NA] NA
[NA] 82.9 (77.2–88.6)
[55.4 (48.1–62.7)] AUC 0.92 (NA)
[0.70 (NA)]
( P = .0001) 0.81 (0.75–0.86)
[0.68 (0.62–0.74)]
( P < .001) 0.90 (0.87–0.94)
[0.81 (0.76–0.87)]
( P = .0008) 0.91
[0.78 (NA)]
( P = .078) NA
[NA] 0.87 (0.77–0.96)
[0.74 (0.62–0.85)]
( P = .0121)
AUC, area under the receiver operating characteristic curve; cCTA, coronary computed tomographic angiography; CI, confidence interval; CT-FFR, fractional flow reserve from coronary computed tomographic angiography; FFR, fractional flow reserve; NA, not available; NPV, negative predictive value; PPV, positive predictive value.
Get Radiology Tree app to read full this article<
Intermediate Stenosis
Get Radiology Tree app to read full this article<

TABLE 5
Per-Vessel Diagnostic Performance of CT-FFR in Patients with Intermediate Luminal Stenosis (30%–70%) According to cCTA ( n = 634)
Koo et al.
(DISCOVER-FLOW) Min et al.
(DeFACTO) Nørgaard et al.
(NXT Trial) Renker et al. Coenen et al. Pooled Substudy Min et al.
Am J Cardiol 2012 Nakazato
Circ Imaging 2013 Number of vessels with intermediate stenosis (30%–70%) 66/159 \*
(41.5%) 150/407
(36.9%) 235/484
(48.6%) 39/67
(58.2%) 144/189
(76.2%) 634/1306
(48.5%) Sensitivity (%) 90 (28–31)
[90 (28–31)] 74 (57–88)
[34 (19–52)] 80 (75–85)
[93 (85–97)] NA 87.3 (76.5–94.3)
[82.5 (70.9–90.9)] 81.4 (70.4–92.3)
[75.3 (27.6–100.0)] Specificity (%) 83 (29–35)
[26 (9–35)] 67 (58–75)
[72 (63–80)] 79 (72–84)
[32 (26–40)] NA 59.3 (47.8–70.1)
[21.0 (12.7–31.5)] 71.7 (54.3–89.0)
[38.8 (25.6–77.5)] PPV (%) 82 (28–34)
[52 (28–54)] 41 (29–54)
[27 (15–43)] 63 (53–72)
[37 (31–44)] NA 62.5 (51.5–72.6)
[44.8 (35.6–54.3)] 59.4 (35.5–83.4)
[38.0 (22.4–53.7)] NPV (%) 91 (29–32)
[75 (9–12)] 90 (81–95)
[78 (69–86)] 92 (87–96)
[91 (81–96)] NA 85.7 (73.8–93.6)
[60.7 [40.6–78.5)] 89.9 (85.0–94.7)
[78.6 (55.4–100.0)] Accuracy (%) 86 (57–66)
[56 (43–68)] 69 (61–76)
[63 (55–71)] 80 (75–85)
[51 (44–57)] NA 71.5 (64.2–78.9)
[47.9 (39.8–56.1)] 75.9 (62.5–89.2)
[55.1 (43.9–66.4)] AUC 0.86 (0.78–0.95)
[0.58 (0.49–0.67)]
( P < .0001) 0.71 (0.62–0.79)
[0.53 (0.44–0.62)]
( P = .0063) 0.79 (0.74–0.85)
[0.63 (0.58–0.67)]
( P < .0001) NA
NA 0.73 (0.66–0.80)
[0.52 (0.45–0.58)]
( P < .0001) 0.76 (0.65–0.88)
[0.57 (0.49–0.66)]
( P = .0027)
AUC, area under the receiver operating characteristic curve; cCTA, coronary computed tomographic angiography; CT-FFR, fractional flow reserve from coronary computed tomographic angiography; DeFACTO, Determination of Fractional Flow Reserve by Anatomic Computed Tomographic Angiography; DISCOVER-FLOW, Diagnosis of Ischemia-Causing Stenoses Obtained via Noninvasive Fractional Flow Reserve; NA, not available; NPV, negative predictive value; NXT, Analysis of Coronary Blood Flow Using CT Angiography, Next Steps; PPV, positive predictive value.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Correlation of CT-FFR with FFR
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. De Cecco C.N., Meinel F.G., Chiaramida S.A., et. al.: Coronary artery computed tomography scanning. Circulation 2014; 129: pp. 1341-1345.
2. Moscariello A., Vliegenthart R., Schoepf U.J., et. al.: Coronary CT angiography versus conventional cardiac angiography for therapeutic decision making in patients with high likelihood of coronary artery disease. Radiology 2012; 265: pp. 385-392.
3. De Bruyne B., Fearon W.F., Pijls N.H., et. al.: Fractional flow reserve-guided PCI for stable coronary artery disease. N Engl J Med 2014; 371: pp. 1208-1217.
4. Koo B.K., Erglis A., Doh J.H., et. al.: Diagnosis of ischemia-causing coronary stenoses by noninvasive fractional flow reserve computed from coronary computed tomographic angiograms. Results from the prospective multicenter DISCOVER-FLOW (Diagnosis of Ischemia-Causing Stenoses Obtained Via Noninvasive Fractional Flow Reserve) study. J Am Coll Cardiol 2011; 58: pp. 1989-1997.
5. Min J.K., Leipsic J., Pencina M.J., et. al.: Diagnostic accuracy of fractional flow reserve from anatomic CT angiography. JAMA 2012; 308: pp. 1237-1245.
6. Norgaard B.L., Leipsic J., Gaur S., et. al.: Diagnostic performance of noninvasive fractional flow reserve derived from coronary computed tomography angiography in suspected coronary artery disease: the NXT trial (Analysis of Coronary Blood Flow Using CT Angiography: Next Steps). J Am Coll Cardiol 2014; 63: pp. 1145-1155.
7. Renker M., Schoepf U.J., Wang R., et. al.: Comparison of diagnostic value of a novel noninvasive coronary computed tomography angiography method versus standard coronary angiography for assessing fractional flow reserve. Am J Cardiol 2014; 114: pp. 1303-1308.
8. Coenen A., Lubbers M.M., Kurata A., et. al.: Fractional flow reserve computed from noninvasive CT angiography data: diagnostic performance of an on-site clinician-operated computational fluid dynamics algorithm. Radiology 2014; 140992:
9. Moher D., Liberati A., Tetzlaff J., et. al.: Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ 2009; 339: pp. b2535.
10. Leipsic J., Abbara S., Achenbach S., et. al.: SCCT guidelines for the interpretation and reporting of coronary CT angiography: a report of the Society of Cardiovascular Computed Tomography Guidelines Committee. J Cardiovasc Comput Tomogr 2014; 8: pp. 342-358.
11. Min J.K., Koo B.K., Erglis A., et. al.: Usefulness of noninvasive fractional flow reserve computed from coronary computed tomographic angiograms for intermediate stenoses confirmed by quantitative coronary angiography. Am J Cardiol 2012; 110: pp. 971-976.
12. Levine G.N., Bates E.R., Blankenship J.C., et. al.: 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention. A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. J Am Coll Cardiol 2011; 58: pp. e44-e122.
13. Cury R.C., Magalhaes T.A., Borges A.C., et. al.: Dipyridamole stress and rest myocardial perfusion by 64-detector row computed tomography in patients with suspected coronary artery disease. Am J Cardiol 2010; 106: pp. 310-315.
14. Techasith T., Cury R.C.: Stress myocardial CT perfusion: an update and future perspective. JACC Cardiovasc Imaging 2011; 4: pp. 905-916.
15. Nakazato R., Park H.B., Berman D.S., et. al.: Noninvasive fractional flow reserve derived from computed tomography angiography for coronary lesions of intermediate stenosis severity: results from the DeFACTO study. Circ Cardiovasc Imaging 2013; 6: pp. 881-889.