
Rationale and Objective
Patients with ulcerative colitis require recurrent conventional colonoscopy (CC) to define the extent of the disease. Computed tomography (CT) colonography (CTC) can be used as an alternative technique for studying the colon in these patients. The purpose of the study was to compare the findings of CTC to CC in patients with ulcerative colitis.
Materials and Methods
Twenty patients proven to have ulcerative colitis on biopsy and in clinical remission state were enrolled in the study. They underwent CTC and CC within 1 week of each test. The investigators performing CTC and CC were blinded to the findings of each other. The chi-square test, kappa test, sensitivity, and specificity were used to compare the findings on CTC and CC. In addition, patient acceptance for both the procedures was compared.
Results
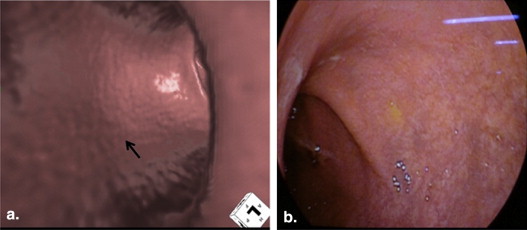
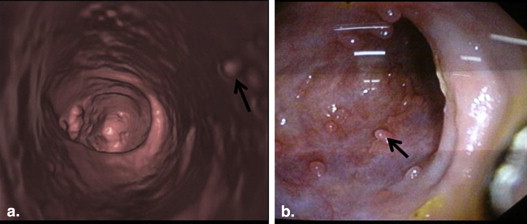
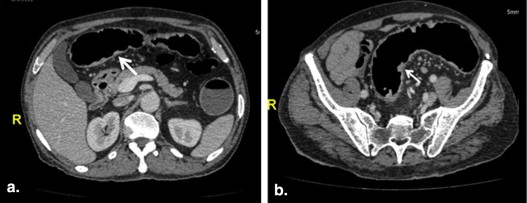
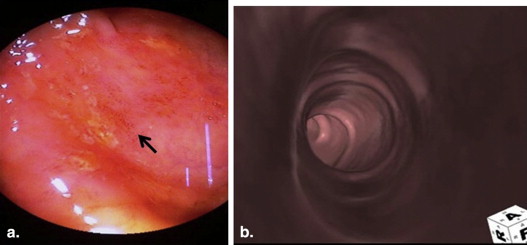
Sensitivity and specificity on CTC for detecting granular appearance were 81.0% and 73.8%, respectively, and for pseudopolyps were 82.1% and 84.5%, respectively. Good correlation was seen between CTC and CC for detection of granular appearance and pseudopolyps. Loss of haustral folds, wall thickening, pericolonic vascularity, and pericolonic lymph nodes seen on CTC were found to correlate with intraluminal findings seen on CC. Patient acceptance for CTC was better than that for CC.
Conclusions
CTC can be used for evaluating patients with ulcerative colitis who are in remission.
Ulcerative colitis is a chronic inflammatory disorder of the bowel of unknown etiology . Patients with ulcerative colitis require recurrent conventional colonoscopy (CC) to define the extent of the disease, to reconfirm the validity of diagnosis, and for cancer surveillance. Computed tomography (CT) colonography (CTC) can be used as an alternative technique for studying the colon. In this technique, volumetric data obtained by high-resolution helical CT are analyzed using specialized computer software to generate virtual colonoscopic images . Its advantage over CC includes its less-invasive nature, ability to visualize the entire colon, absence of blind areas, and evaluation of extracolonic pathology. It allows simultaneous assessment of colonic mucosal surface, wall thickness, surrounding structures, local lymphadenopathy, fistulae, and evaluation of proximal colon in patients with obstructive stricture. CTC is able to identify endoluminal, intramural, and extracolonic findings. To the best of our knowledge, this is the first study in English literature which evaluates the use of 64-slice CTC in patients with ulcerative colitis. The correlation between CTC and CC for granular appearance and pseudopolyps has been evaluated in this study.
Materials and methods
Twenty consecutive patients of either sex, presenting to the Gastroenterology Department, proven to have ulcerative colitis on colonoscopic or sigmoidoscopic biopsy, and presently in clinically remission state, were enrolled in the study. The institutional ethics committee approved the study protocol, and an informed consent was obtained from each patient. Exclusion criteria included 1) age <18 years, 2) patients having active ulcerative colitis, and 3) allergy from contrast media. Three days before CTC, patients were asked to eat food with low fiber content. Patients were given wet preparation. Wet preparation included two packets of polyethylene glycol electrolyte solution (Peglec; Tablets Limited) dissolved in 2 L of water, given 12 hours before the study. Forty milliliters of 76% Diatrizoate Megulamine & Diatrizoate Sodium iodinated contrast (Trazograf 76%; Unique pharmaceuticals) was added to the Peglec solution, for the effective differentiation of fecal material from polyps. To achieve adequate bowel distention during CTC, injection hyoscine N-butylbromide (Buscopan; German Remedies Limited) 20 mg was given intravenously to all patients, who did not have history of glaucoma or urinary retention due to high-grade prostate enlargement.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
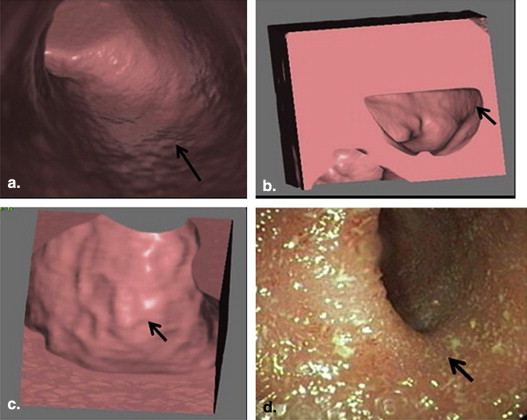
Table 1
Table Showing Frequency of Intraluminal Findings (Granular Appearance and Pseudopolyps) on CTC and CC, and Association of Findings of CTC and CC with Each Other
Intraluminal findings on CTC and CC Percentage of Colon Segments Involved on CTC Percentage of Colon Segments Involved on CC Association Between CTC and CC_P_ Value (Chi-Square Test) Cohen Kappa Coefficient Granular appearance 56.1 56.4 <.001 0.550 Pseudopolyps 28.4 22.1 <.001 0.566
CC, conventional colonoscopy; CTC, computed tomography colonography.
Moderate agreement was seen between them.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Table Showing Frequency of Extraluminal Findings on CTC and Their Association with Endoluminal Findings on CC
Extraluminal Findings on CTC Percentage of Colon Segments Involved on CTC Endoluminal Findings on CC Association Between the Extraluminal Findings on CTC and Endoluminal Findings on CC_P_ Value (Chi-Square Test) Cohen Kappa Coefficient Loss of haustral folds 48.8 Loss of vascular pattern <.01 0.677 Granular appearance <.01 0.623 Increased wall thickness 46.3 Loss of vascular pattern <.01 0.572 Granular appearance <.01 0.546 Increased pericolonic vascularity 61.3 Loss of vascular pattern <.01 0.313 Granular appearance <.01 0.329 Increased pericolonic lymph nodes 40.0 Loss of vascular pattern <.01 0.390 Granular appearance <.01 0.369
CC, conventional colonoscopy; CTC, computed tomography colonography.
Fair to substantial agreement was seen between them.

Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. MacKalski B.A., Bernstein C.N.: New diagnostic imaging tools for inflammatory bowel disease. Gut 2006; 55: pp. 733-741.
2. Herfarth H., Schreyer A.G.: The virtuosity of virtuality or how real is virtual colonography. Gut 2003; 52: pp. 1662-1664.
3. Kattan K.R., King A.Y.: Presacral space revisited. AJR Am J Roentgenol 1979; 132: pp. 437-439.
4. Jung H.S., Park D.K., Kim M.J., et. al.: A comparison of patient acceptance and preferences between CT colonography and conventional colonoscopy in colorectal cancer screening. Korean J Intern Med 2009; 24: pp. 43-47.
5. Vining D.J., Gelfand D.W., Bechtold R.E., et. al.: Technical feasibility of colon imaging with helical CT and virtual reality [Abstract]. AJR Am J Roentgenol 1994; 62: pp. 10.
6. Kim S.H., Choi B.I., Han J.K., et. al.: CT colonography in a Korean population with a high residue diet: comparison between wet and dry preparations. Clin Radiol 2006; 61: pp. 483-494.
7. Nagata K., Singh A.K., Sangwaiya M., et. al.: Comparative evaluation of the fecal-tagging quality in CT colonography: barium vs. iodinated oral contrast agent. Acad Radiol 2009; 16: pp. 1393-1399.
8. Chen S.C., Lu D.S., Hecht J.R., et. al.: CT colonography: value of scanning in both the supine and prone positions. AJR Am J Roentgenol 1999; 172: pp. 595-599.
9. Kalra N., Suri S., Bhasin D.K., et. al.: Comparison of multidetector computed tomographic colonography and conventional colonoscopy for detection of colorectal polyps and cancer. Indian J Gastroenterol 2006; 25: pp. 229-232.
10. Bhatia A., Saxena A.K., Kalra N., et. al.: Intravenous contrast enhanced computed tomography colonoscopy in children with suspected colonic polyps. Eur J Radiol 2013; 82: pp. 905-912.
11. Taylor S.A., Halligan S., Goh V., et. al.: Optimizing colonic distention for multi-detector row CT colonography: Effect of hyoscine butylbromide and rectal balloon catheter. Radiology 2003; 229: pp. 99-108.
12. Itzkowitz S.H.: Colonic polyps and polyposis syndromes.2002.WB Saunders CompanyPhiladelphia, Pennsylvania:pp. 2175-2214.
13. Carrascosa P., Castiglioni R., Capun˜ay C., et. al.: CT colonoscopy in inflammatory bowel disease. Abdom Imaging 2007; 32: pp. 596-601.
14. Andersen K., Vogt C., Blondin D., et. al.: Multi-detector CT-colonography in inflammatory bowel disease: prospective analysis of CT-findings to high-resolution video colonoscopy. Eur J Radiol 2006; 58: pp. 140-146.
15. Yucel C., Lev-Toaff A.S., Moussa N., et. al.: CT colonography for incomplete or contraindicated optical colonoscopy in older patients. AJR Am J Roentgenol 2008; 190: pp. 145-150.
16. Lefere P., Gryspeerdt S., Baekelandt M., et. al.: Diverticular disease in CT colonography. Eur Radiol 2003; 13: pp. L62-L74.
17. Gilat T., Fireman Z., Grossman A., et. al.: Colorectal cancer in patients with ulcerative colitis. A population study in central Israel. Gastroenterology 1998; 94: pp. 870-877.
18. Gyde S.N., Prior P., Allan R.N., et. al.: Colorectal cancer in ulcerative colitis: a cohort study of primary referrals from three centres. Gut 1988; 29: pp. 206-217.
19. Moody G.A., Jayanthi V., Probert C.S., et. al.: Long-term therapy with sulphasalazine protects against colorectal cancer in ulcerative colitis: A retrospective study of colorectal cancer risk and compliance with treatment in Leicestershire. Eur J Gastroenterol Hepatol 1996; 8: pp. 1179-1183.
20. Coady F.L., Angel L.P., Procaccino J.A.: Perforated colon secondary to virtual colonoscopy: report of a case. Dis Colon Rectum 2004; 7: pp. 1247-1249.
21. Kamar M., Portnoy O., Bar-Dayan A., et. al.: Actual colonic perforation in virtual colonoscopy: report of a case. Dis Colon Rectum 2004; 47: pp. 1242-1244.
22. Siewart Bettina, Jonathan B., Eisenberg R., et. al.: Quality initiatives: quality improvement grand rounds at Beth Israel Deaconess Medical Center: CT colonography performance review after an adverse event. RadioGraphics 2010; 30: pp. 23-31.