
Rationale and Objectives
To evaluate different techniques for reducing hemorrhagic complications in coagulopathic patients with elevated international normalized ratio having an image-guided percutaneous invasive procedure; techniques included systemic transfusion of fresh frozen plasma (FFP), local injection of FFP, percutaneous injection of gelatin sponge, and percutaneous placements of angiographic coils.
Materials and Methods
Retrospective review of 232 consecutive patients with known coagulopathy undergoing image-guided minimally invasive procedures were selected. Ninety-one patients had local FFP injected, 40 patients underwent local synthetic gelatin injection, 16 patients had percutaneous coil embolization, and 85 patients received systemic FFP. The number of bleeds, complications related to bleeds, and systemic complications were recorded. A 30 cc threshold was used to delineate significant bleeding.
Results
No patients experienced clinically significant or insignificant bleeding with local FFP injection ( P value <.05). Other local hemostatic methods (Gelfoam, systemic FFP, and coil embolization) were associated with higher levels of bleeding (12.5%, 17.1%, 37.5%, respectively) and complications (7.5%, 31.4%, 37.5%, respectively). Systemic FFP infusion was associated with respiratory, infectious, and mortal complications.
Conclusions
Local injection of blood products provides a safe and efficacious hemostatic agent to reduce the incidence of postprocedural bleeding. The technique is associated with lower rates of bleeding and systemic complications when compared to other local and systemic techniques. Further randomized prospective studies with a larger patient cohort need to be performed to corroborate these initial findings.
Introduction
Patients presenting with an elevated international normalized ratio (INR) or other clotting factor abnormalities are at risk of bleeding when undergoing a variety of procedures, and this bleeding may be difficult to detect . Bleeding can present a unique problem to interventional radiologists as the minimally invasive nature of the procedures precludes direct visualization of bleeding and subsequent hemostatic maneuvers possible in open surgical procedures. Bleeding from interventional procedures can present insidiously and unexpectedly . Percutaneous biopsies of solid organs can result in high major bleeding rates in patients with an elevated INR . It is therefore important for clinicians to know methods to mitigate risk and provide procedures to patients with coagulopathy.
Traditionally, risk remediation in patients with elevated INR is performed with intravenous infusions of fresh frozen plasma (FFP), which helps reverse elevated INR values by providing systemic clotting factors. This approach may not mitigate significant bleeding risk, as studies have shown large volume transfusions have no significant effect on bleeding outcomes . Large volume infusions carry the risk of transfusion-related reactions, infections, and volume overload, especially in patients with significant comorbidities such as congestive heart disease . The cost of blood products can be more substantial when given in larger volumes and when added to the cost of testing patient compatibility . Despite the narrow indications for FFP, there is widespread use of FFP largely attributed to procedural preparation .
Get Radiology Tree app to read full this article<
Methods
Get Radiology Tree app to read full this article<
Patient Demographics
Get Radiology Tree app to read full this article<
TABLE 1
Demographics
Local FFP Gelfoam Systemic FFP Local Coils Total number of patients 91 40 85 16 Males 43 (47.3%) 17 (42.5%) 52 (61.1%) 9 (56.3%) Average age 53 50 49 56 Average INR 2.24 (range 2–3) 2.32 (range 2.1–2.9) 2.45 (range 2.4–3.4) 2.3 Number of patients on coumadin 18 (19.8%) 25 (62.5%) 12 (14.1%) 4 (25%) Average product injected 20 cc (range 5–30 cc) (corresponding to 20 mg) Unknown 5.2 units (range 1–26) 2 coils
TABLE 2
Types of Procedures
Local FFP Gelfoam Systemic FFP Local Coils Liver biopsy 43 (47%) 26 (65%) 33 (39%) 8 (50%) Lung biopsy 7 (8%) 0 1 (1%) 0 Soft tissue biopsy (nonrenal) 8 (9%) 10 (25%) 12 (14%) 1 (6%) Drainage 17 (19%) 4 (10%) 24 (28%) 0 Cholangiogram/Cholecystostomy 4 (4%) 0 3 (4%) 0 Renal biopsy 8 (9%) 0 3 (4%) 7 (44%) Chest tube placement 4 (4%) 0 9 (11%) 0 TOTAL 91 40 85 16
TABLE 3
Reason for Coagulopathy
Local FFP Gelfoam Systemic FFP Local Coils Coumadin 47 (52%) 25 (63%) 41 (48%) 7 (44%) Other anticoagulants 5 (5%) 0 10 (12%) 5 (31%) Liver failure 25 (27%) 7 (18%) 21 (25%) 0 Hematologic malignancy 7 (8%) 1 (3%) 13 (15%) 2 (13%) Chemotherapy 3 (3%) 2 (5%) 10 (12%) 0 Idiopathic 4 (4%) 5 (13%) 20 (24%) 2 (13%)
Get Radiology Tree app to read full this article<
Injection Method
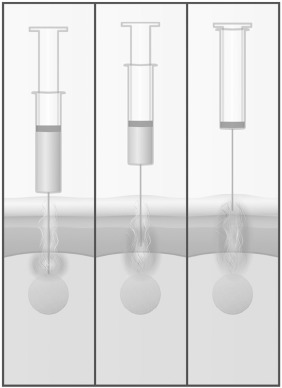
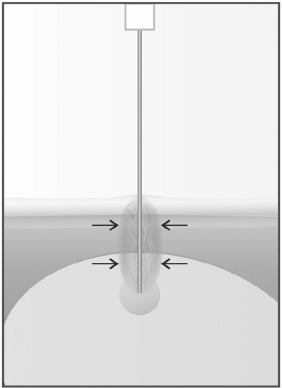
Local Injection of Blood Elements Technique
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Gelfoam Technique
Get Radiology Tree app to read full this article<
Coil Technique
Get Radiology Tree app to read full this article<
Intravenous FFP Technique
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
TABLE 4
Bleeding Rates
Local FFP Gelfoam Systemic FFP Local Coils All type bleeding rate 0% 17.5% 16.5% 37.5% Clinical significant bleeding rate 0% 12.5% 7.1% 37.5% Total number of clinically insignificant bleeds 0 2 8 0 Total number of clinically significant bleeds 0 5 6 6 Total number of nonbleeding complications 0 0 6 0 Total complication rate related to procedure 0% 17.5% 23.5% 37.5%
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
TABLE 5
Additional Complications
Local FFP Gelfoam Systemic FFP Local Coils Shortness of breath 0 0 1 0 Shortness of breath requiring intubation or other treatment 0 0 1 0 Infection 0 0 1 0 Death related to volume overload or transfusion reaction 0 0 3 0
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Patel I.J., Davidson J.C., Nikolic B., et. al.: Consensus guidelines for periprocedural management of coagulation status and hemostasis risk in percutaneous image-guided interventions. J Vasc Interv Radiol 2012; 23: pp. 727-736.
2. Amarapurkar P.D., Amarapurkar D.N.: Management of coagulopathy in patients with decompensated liver cirrhosis. Int J Hepatol 2011; 2011: pp. 695470.
3. Yang L., Stanworth S., Hopewell S., et. al.: Is fresh-frozen plasma clinically effective? An update of a systematic review of randomized controlled trials. Transfusion 2012; 52: pp. 1673-1686. quiz 1673
4. Thampanitchawong P., Piratvisuth T.: Liver biopsy: complications and risk factors. World J Gastroenterol 1999; 5: pp. 301-304.
5. Grant A., Neuberger J.: Guidelines on the use of liver biopsy in clinical practice. British Society of Gastroenterology. Gut 1999; 45:
6. Darcy M.D., Kanterman R.Y., Kleinhoffer M.A., et. al.: Evaluation of coagulation tests as predictors of angiographic bleeding complications. Radiology 1996; 198: pp. 741-744.
7. Thachil J.: Abnormal coagulation tests before kidney biopsies—what next?. Clin Kidney J 2013; 6: pp. 50-54.
8. Muller M.C., Arbous M.S., Spoelstra-de Man A.M., et. al.: Transfusion of fresh-frozen plasma in critically ill patients with a coagulopathy before invasive procedures: a randomized clinical trial (CME). Transfusion 2015; 55: pp. 26-35. quiz 25
9. Pandey S., Vyas G.N.: Adverse effects of plasma transfusion. Transfusion 2012; 52: pp. 65S-79S.
10. Mannuci P.M.: Abnormalities of haemostasis tests in chronic liver disease: clinically relevant?. Portal Hypertens 2008; 15: pp. 40-46.
11. Haaga J., Rahim S.: Direct injection of blood products versus gelatin sponge as a technique for local hemostasis. Cardiovasc Intervent Radiol 2017; 40: pp. 231-235.
12. Dzik W., Rao A.: Why do physicians request fresh frozen plasma?. Transfusion 2004; 44: pp. 1393-1394.
13. Wallis J.P., Dzik S.: Is fresh frozen plasma overtransfused in the United States?. Transfusion 2004; 44: pp. 1674-1675.
14. Lin Y., Foltz L.: Proposed guidelines for platelet transfusion. BCMJ 2005; 47: pp. 245-248.
15. Chuang V.P., Alspaugh J.P.: Sheath needle for liver biopsy in high-risk patients. Radiology 1988; 166: pp. 261-262.
16. Laeseke P.F., Winter T.C., Davis C.L., et. al.: Postbiopsy bleeding in a porcine model: reduction with radio-frequency ablation—preliminary results. Radiology 2003; 227: pp. 493-499.
17. Chowdary P., Saayman A.G., Paulus U., et. al.: Efficacy of standard dose and 30 ml/kg fresh frozen plasma in correcting laboratory parameters of haemostasis in critically ill patients. Br J Haematol 2004; 125: pp. 69-73.
18. Nakamoto D.A., Wilkins L.R., Haaga J.R.: Hemostasis effects of direct intraparenchymal injection of platelets and fresh frozen plasma before cutting needle biopsy in an animal model. J Vasc Interv Radiol 2011; 22: pp. 1601-1605.
19. Falstrom J.K., Moore M.M., Caldwell S.H., et. al.: Use of fibrin sealant to reduce bleeding after needle liver biopsy in an anticoagulated canine model: work in progress. J Vasc Interv Radiol 1999; 10: pp. 457-462.
20. Warner M.A., Woodrum D.A., Hanson A.C., et. al.: Prophylactic plasma transfusion before interventional radiology procedures is not associated with reduced bleeding complications. Mayo Clin Proc 2016; 91: pp. 1045-1055.
21. Hussein M.A., Hoeltge G.A.: Platelet transfusion therapy for medical and surgical patients. Cleve Clin J Med 1996; 63: pp. 245-250.
22. Warner M.A., Jia Q., Clifford L., et. al.: Preoperative platelet transfusions and perioperative red blood cell requirements in patients with thrombocytopenia undergoing noncardiac surgery. Transfusion 2016; 56: pp. 682-690.
23. Atar E., Ben Ari Z., Bachar G.N., et. al.: A comparison of transjugular and plugged-percutaneous liver biopsy in patients with contraindications to ordinary percutaneous liver biopsy and an “in-house” protocol for selecting the procedure of choice. Cardiovasc Intervent Radiol 2010; 33: pp. 560-564.
24. Dasararaju R., Marques M.B.: Adverse effects of transfusion. Cancer Control 2015; 22: pp. 16-25.