
Rationale and Objectives
To measure main pancreatic duct diameter (PDD) with magnetic resonance pancreatography (MRP) before and after secretin injection in patients with suspected sphincter of Oddi dysfunction (SOD) and to determine if the diameter change is predictive of sphincter of Oddi manometry (SOM) results.
Materials and Methods
We identified all patients during the study period referred for SOM for clinically suspected SOD; patients with an intact sphincter and without contraindication to MRP examination were considered for study entry. Consenting patients underwent MRP, including dynamic imaging of the pancreatic duct after intravenous administration of porcine secretin followed by SOM during endoscopic retrograde cholangiopancreatography. MRP was defined as abnormal when PDD remained increased by ≥1.0 mm from baseline 15 minutes after secretin injection. SOM was abnormal when basal sphincter pressure (SP) was ≥40 mm Hg. Mean PDD before and after secretin administration was compared within normal and abnormal SP groups with two-tailed unpaired t -test; the mean difference between baseline and peak PDD and duration of ≥0.5 mm increase in PDD was compared between groups with two-tailed t -test. P < .05 was considered significant.
Results
Of 70 patients referred for SOM, 30 met all entry criteria, gave consent to participate, and underwent both MRP and SOM. Ten of 30 patients (33%) had normal SP; 20 (67%) were abnormal. PDD increased significantly after secretin injection (normal SP, 1.62 ± 0.73 to 2.78 ± 0.77 mm, P < .01; abnormal SP, 1.45 ± 0.26 to 2.32 ± 0.75 mm, P < .01). There was no difference between normal and abnormal SP groups in amount of PDD increase (1.15 ± 0.75 vs. 0.88 ± 0.72 mm; P = .33) or duration of ≥0.5 mm increase in PDD (5.28 ± 8.76 vs. 13.60 ± 13.00 minutes; P = 0.07).
Conclusions
In patients with suspected sphincter of Oddi dysfunction, magnetic resonance pancreatography demonstrated PDD increase following secretin injection but did not predict the results of manometry.
Sphincter of Oddi dysfunction (SOD) is increasingly recognized as a cause for upper abdominal pain and idiopathic pancreatitis ( ). Sphincter of Oddi manometry (SOM) is the reference standard for the diagnosis of SOD and can be performed by endoscopic retrograde cholangiopancreatography (ERCP), transcutaneously (usually via a T-tube tract), or intraoperatively. A basal sphincter pressure ≥40 mm Hg is considered abnormal ( ).
However, SOM is a costly, invasive procedure that is not widely available and is associated with significant morbidity (e.g., post-ERCP pancreatitis) ( ). Consequently, several less-expensive and less-invasive tests have been evaluated, including morphine-prostigmine provocative test (Nardi test) and quantitative hepatobiliary scintigraphy. Unfortunately, each of these tests has limitations. The Nardi test has low sensitivity and specificity in predicting the presence of SOD ( ). Compared to SOM as the reference standard, two recent reports showed hepatobiliary scintigraphy has a sensitivity of only 25% to 49% and a specificity of 78% to 90% for diagnosing SOD ( ). Furthermore, hepatobiliary scintigraphy does not image the pancreatic duct.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Get Radiology Tree app to read full this article<
Magnetic Resonance Pancreatography
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Endoscopic Retrograde Cholangiopancreatography/Sphincter of Oddi Manometry
Get Radiology Tree app to read full this article<
Image Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Demographic Characteristics and Procedure Indications between Normal and Abnormal Pancreatic Manometry Groups
Normal SOM Abnormal SOM_P_ -Value Number 10 20 Male/female 4/6 4/16 .38 Mean (SD) age (y) 54 (17) 48 (13) .26 Indication Idiopathic recurrent AP 3 (30%) 5 (25%) 1.00 Single episode AP 0 2 (10%) .54 Abdominal pain without AP 7 (70%) 13 (65%) 1.00 Clinical SOD classification type II 5 (50%) 12 (60%) .71 Clinical SOD classification type III 5 (50%) 8 (40%) .71 Prior cholecystectomy 5 (50%) 9 (45%) 1.00
AP: acute pancreatitis; SOD: sphincter of Oddi dysfunction; SOM: sphincter of Oddi manometry.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Main Pancreatic Duct (PD) Diameter (mm) and Percent Change From Baseline Before and at Various Time Points (minutes) After Secretin Stimulation
SOM N 0 1 2 3 4 5 6 7 10 15 20 30 Normal 10 1.62 1.95 2.78 2.50 2.40 2.19 2.20 2.10 1.91 2.00 1.80 2.00 (20%) (71%) (54%) (48%) (35%) (36%) (30%) (18%) (24%) (11%) (24%) Abnormal 20 1.45 1.82 2.00 2.32 2.02 1.70 1.84 1.68 1.52 1.49 1.57 1.53 (26%) (38%) (61%) (39%) (17%) (27%) (16%) (5%) (3%) (8%) (6%) Overt CP* 9 2.17 2.58 2.82 3.07 2.70 2.63 2.58 2.48 2.33 2.29 2.35 2.38 (19%) (30%) (41%) (24%) (21%) (19%) (14%) (7%) (6%) (8%) (10%)
CP: chronic pancreatitis.
Overt CP was defined as mild to severe chronic pancreatitis change by ERCP, according to the Cambridge classification.
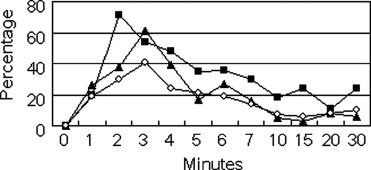
![Figure 2, Mean caliber of the main pancreatic duct before (0 minutes) and 1, 2, 3, 4, 5, 6, 7, 10, 15, 20, and 30 minutes after the administration of secretin in patients with normal (■) and abnormal (▲) pancreatic manometry results. With secretin stimulation, both groups have statistically significant dilation of the main pancreatic ductal diameters from baseline ( P < .01 [■], P < .01 [▲].](https://storage.googleapis.com/dl.dentistrykey.com/clinical/ComparisonofSecretinStimulatedMagneticResonancePancreatographyandManometryResultsinPatientswithSuspectedSphincterofOddiDysfunction/1_1s20S107663320700712X.jpg)
Table 3
Mean (SD) Pancreatic Ductal Diameter Before and After Secretin Administration for Patients with Normal Pancreatic Sphincter of Oddi Manometry (SOM), Abnormal SOM, and Overt Chronic Pancreatitis (CP) ⁎
Normal SOM a (n = 10) Abnormal SOM b (n = 20) Overt CP c (n = 9) Presecretin 1.62 (0.73) 1.45 (0.26) 2.17 (0.94) Maximum postsecretin 2.78 (0.77) 2.32 (0.75) 3.07 (1.19) Percent increase 71% 61% 41%
P- Values for comparisons of change in mean diameter were .33 (a vs b), .54 (a vs c), and .92 (b vs c).
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 4
Comparison of Means (SDs) of Main Pancreatic Duct (PD) Measurements Between Patients with Normal and Abnormal sphincter of Oddi Manometry (SOM) Results
Normal SOM (n = 10) Abnormal SOM (n = 20)P -Value Presecretin diameter (mm) 1.62 (0.73) 1.45 (0.26) .33 Maximum postsecretin diameter (mm) 2.78 (0.77) 2.32 (0.75) .13 Maximum diameter change (mm) 1.15 (0.70) 0.88 (0.72) .33 Time to maximum diameter (min) 2.51 (1.02) 2.89 (1.57) .52 Time to ≥0.5-mm change (min) 1.38 (0.52) 1.80 (1.14) .33 Duration of >0.5-mm change (min) 13.60 (13.00) 5.28 (8.76) .07
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 5
Pancreatic Duct Response to Secretin (MRCP) versus Sphincter of Oddi manometry (SOM) for Diagnosis of Sphincter of Oddi Dysfunction
MRCP SOM Normal Abnormal Total Normal 9 18 27 Abnormal 1 2 3 Total 10 20 30
MRCP sensitivity = 10%; MRCP specificity = 90%.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 6
Duodenal Filling Grade Among Normal Pancreatic Sphincter of Oddi Manometry (SOM), Abnormal SOM, and Overt Chronic Pancreatitis (CP) Patients
Grade Normal SOM (n = 10) Abnormal SOM (n = 20) Overt CP (n = 9) 1 0 0 0 2 1 (10%) 2 (10%) 3 (33%) 3 9 (90%) 18 (90%) 6 (67%)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Summary
Get Radiology Tree app to read full this article<
References
1. Della Libera E., Rodrigues R.A., Guimaraes A.P., Paulo G.A., Geocze S., Ferrari A.P.: Prevalence of sphincter of Oddi dysfunction in patients referred to endoscopic retrograde cholangiopancreatography. Arq Gastroenterol 2007; 44: pp. 18-21.
2. Coyle W.J., Pineau B.C., Tarnasky P.R., et. al.: Evaluation of unexplained acute and acute recurrent pancreatitis using endoscopic retrograde cholangiopancreatography, sphincter of Oddi manometry and endoscopic ultrasound. Endoscopy 2002; 34: pp. 617-623.
3. Corazziari E.: Sphincter of Oddi dysfunction. Dig Liver Dis 2003; 35: pp. S26-S29.
4. Guelrud M., Mendoza S., Rossiter G., et. al.: Sphincter of Oddi manometry in healthy volunteers. Dig Dis Sci 1990; 35: pp. 38-46.
5. Wong G.S., Teoh N., Dowsett J.D., Bell C.J., Kellow J.E.: Complications of sphincter of Oddi manometry: Biliary-like pain versus acute pancreatitis. Scand J Gastroenterol 2005; 40: pp. 147-153.
6. Maldonado M.E., Brady P.G., Mamel J.J., Robinson B.: Incidence of pancreatitis in patients undergoing sphincter of Oddi manometry (SOM). Am J Gastroenterol 1999; 94: pp. 387-390.
7. Scicchitano J., Saccone G.T., Baker R.A., Roberts-Thomson I.C., Toouli J.: How safe is endoscopic sphincter of Oddi manometry?. J Gastroenterol Hepatol 1995; 10: pp. 334-336.
8. Steinberg W.M., Salvato R.F., Toskes P.P.: The morphine-prostigmin provocative test: Is it useful for making clinical decisions?. Gastroenterology 1980; 78: pp. 728-731.
9. Rosenblatt M.L., Catalano M.F., Alcocer E., et. al.: Comparison of sphincter of Oddi manometry, fatty meal sonography, and hepatobiliary scintigraphy in the diagnosis of sphincter of Oddi dysfunction. Gastrointest Endosc 2001; 54: pp. 697-704.
10. Craig A.G., Peter D., Saccone G.T., et. al.: Scintigraphy versus manometry in patients with suspected biliary sphincter of Oddi dysfunction. Gut 2003; 52: pp. 352-357.
11. Geenen G.E., Hogan W.J., Dodds W.J., et. al.: Intraluminal pressure recording from the human sphincter of Oddi. Gastroenterology 1980; 78: pp. 317-324.
12. Carr-Locke D.L., Gregg J.A., Chey W.Y.: Effects of exogenous secretin on pancreatic and biliary ductal and sphincteric pressures in man demonstrated by endoscopic manometry and correlation with plasma secretin levels. Dig Dis Sci 1985; 30: pp. 909-917.
13. Bolondi L., Gaiani S., Gullo L., et. al.: Secretin administration induces a dilatation of main pancreatic duct. Dig Dis Sci 1984; 29: pp. 802-808.
14. Glaser J., Hogemann B., Krummenerl T., et. al.: Sonographic imaging of the pancreatic duct: new diagnostic possibilities using secretin stimulation. Dig Dis Sci 1987; 32: pp. 1075-1081.
15. Glaser J., Hogemann B., Schneider M., et. al.: Significance of a sonographic secretin test in diagnosis of pancreatic disease. Scand J Gastroenterol 1989; 24: pp. 179-185.
16. Cavallini G., Rigo L., Bovo P., et. al.: Abnormal US response of main pancreatic duct after secretin administration in patients with acute pancreatitis of different etiology. J Clin Gastroenterol 1994; 18: pp. 298-303.
17. Warshaw A.L., Simeone J., Schapiro A.H., et. al.: Objective evaluation of ampullary stenosis with ultrasonography and pancreatic stimulation. Am J Surg 1985; 149: pp. 65-72.
18. Matos C., Metens T., Deviere J., et. al.: Pancreatic duct: Morphological and functional evaluation with dynamic MR pancreatography after secretin stimulation. Radiology 1997; 203: pp. 435-441.
19. Troiano F., O’Connor K., Lehman G., et. al.: Comparison of secretin-stimulated ultrasound and sphincter of Oddi manometry in evaluating sphincter of Oddi dysfunction. Gastrointest Endosc 1989; 35: pp. A166.
20. Di Francesco V., Brunori M.P., Rigo L., et. al.: Comparison of ultrasound-secretin test and sphincter of Oddi manometry in patients with recurrent acute pancreatitis. Dig Dis Sci 1999; 44: pp. 336-340.
21. Catalano M.F., Lahoti S., Alcocer E., et. al.: Dynamic imaging of the pancreas using real-time endoscopic ultrasonography with secretin stimulation. Gastrointest Endosc 1998; 48: pp. 580-587.
22. Manfredi R., Costamagna G., Brizi M.G., et. al.: Severe chronic pancreatitis versus suspected pancreatic disease: Dynamic cholangiopancreatography after secretin stimulation. Radiology 2000; 214: pp. 849-855.
23. Cappeliez O., Delhaye M., Deviere J., et. al.: Chronic pancreatitis: Evaluation of pancreatic exocrine function with MR pancreatography after secretin stimulation. Radiology 2000; 215: pp. 358-364.
24. Mariani A., Curioni S., Zanello A., et. al.: Secretin MRCP and endoscopic pancreatic manometry in the evaluation of sphincter of Oddi function: A comparative pilot study in patients with idiopathic recurrent pancreatitis. Gastrointest Endosc 2003; 58: pp. 847-852.
25. Khalid A., Peterson M., Slivka A.: Secretin-stimulated magnetic resonance pancreaticogram to assess pancreatic duct outflow obstruction in evaluation of idiopathic acute recurrent pancreatitis. Dig Dis Sci 2003; 48: pp. 1475-1481.
26. Somogyi L., Cintron M., Toskes P.P.: Synthetic porcine secretin is highly accurate in pancreatic function testing in individuals with chronic pancreatitis. Pancreas 2000; 21: pp. 262-265.
27. Lehman G.A., Sherman S.: Sphincter of Oddi dysfunction.Yamada T.Alpers D.H.Laine L.Textbook of Gastroenterology.2003.Lippincott Williams & WilkinsPhiladelphia:pp. 2251-2262.
28. Axon A.T.R., Classen M., Cotton P.B., et. al.: Pancreatography in chronic pancreatitis: international definitions. Gut 1984; 25: pp. 1107-1112.
29. Tarnasky P.R., Hoffman B., Aabakken L., et. al.: Sphincter of Oddi dysfunction is associated with chronic pancreatitis. Am J Gastroenterol 1997; 92: pp. 1125-1129.
30. Bolondi L., Li Bassi S., Gaiani S., et. al.: Impaired response of main pancreatic duct to secretin stimulation in early chronic pancreatitis. Dig Dis Sci 1989; 34: pp. 834-840.