
Rationale and Objectives
To investigate the impact of iterative reconstruction in image space (IRIS) on image noise, image quality (IQ), and postprocessing at coronary computed tomography angiography (cCTA) compared to traditional filtered back-projection (FBP).
Materials and Methods
The cCTA results of 50 patients (26 men; 58 ± 15 years, body mass index 31.5 ± 6.7 kg/m²) were investigated using a second-generation dual-source computed tomography system. Scan data were reconstructed with the use of IRIS and FBP algorithms. Two radiologists independently evaluated the reconstructions using automated coronary tree analysis software. Image noise was measured and IQ was rated on a 5-point Likert scale. The number of manual corrections after automated vessel segmentation, the time required to complete segmentation, and the number of missed segments were assessed in both IRIS and FBP reconstructions. Results were compared using paired t-test .
Results
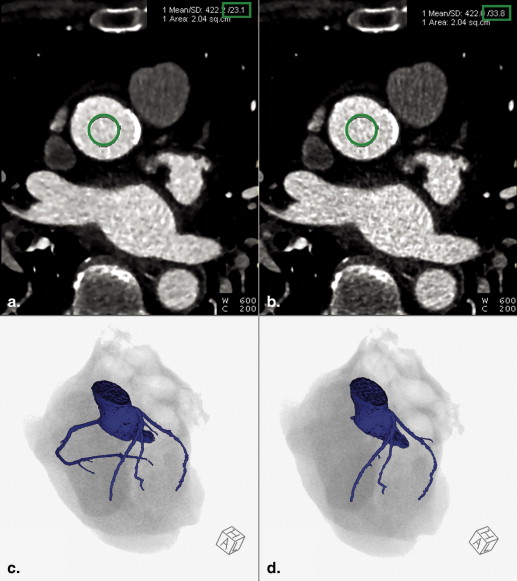
IRIS significantly reduced image noise compared to FBP (23.3 ± 8.8 vs. 33.5 ± 13.5 Hounsfield units, P < .001). Subjective IQ improved with IRIS (IRIS 3.2 ± 1.0 vs. FBP 3.0 ± 1.0, P < .05). IRIS decreased the time needed for coronary segmentation from 111.9 ± 40.5 seconds to 95.2 ± 38.2 seconds with FBP ( P < .01) and required fewer manual corrections (5.7 ± 3.0 vs. 6.8 ± 3.6, P < .01). The number of missed vessel segments was not significantly different (3.6 ± 1.8 vs. 3.8 ± 1.9, P > .05) between IRIS and FBP, respectively.
Conclusions
During cCTA postprocessing, IRIS significantly decreases the time and the number of manual corrections for a complete coronary segmentation compared to FBP. This effect is likely attributable to suppression of image noise by IRIS, which improves the performance of automated vessel segmentation and positively impacts cCTA analysis.
Coronary computed tomography angiography (cCTA) has emerged as a powerful noninvasive modality for the evaluation of coronary artery disease (CAD) in patients with low-to-intermediate pretest likelihood . The thin sections used to evaluate small coronary details at cCTA are inherently more susceptible to increased image noise than are thicker-section routine body examinations. Due to the well-known tradeoffs between radiation dose, image noise, and spatial resolution, low-dose radiation protocols aggravate this relationship and possibly lower diagnostic image quality. .
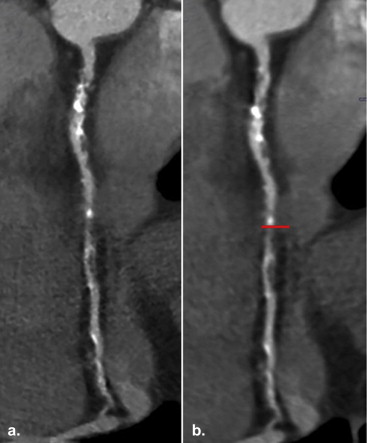
A mainstay of contemporary cCTA image interpretation is image postprocessing using dedicated analysis software for generating curved multiplanar reformats (cMPR) of the vessel course and for addressing other diagnostic aspects obtainable from cCTA. Inaccurate attenuation classification of voxels due to image noise holds the potential to interfere with successful postprocessing, which requires time-consuming manual adjustments. Many studies have investigated the use of postprocessing technique, reconstruction method, and automated and semiautomated segmentation software across a variety of fields and organ systems and with different modalities to determine the possible benefits that can be achieved .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Patients
Get Radiology Tree app to read full this article<
Scanning Technique and Image Reconstruction
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Image Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Patients and Scan Acquisition Protocol
Get Radiology Tree app to read full this article<
Table 1
Patient Demographic and cCTA Acquisition Characteristics
Male 26 (52) Age (years) 58.1 ± 14.8 Weight (kg) 90.8 ± 19.1 Height (cm) 170.0 ± 8.9 BMI (kg/m 2 ) 31.5 ± 6.7 Heart rate (bpm) 70.9 ± 14.6 Tube potential (kVp) 116.8 ± 8.4 Tube current (mAs) 329.5 ± 26.4z -axis coverage (cm) 16.1 ± 3.7 DLP (mGy × cm) 586.9 ± 378.4 CTDIvol (mGy) 36.2 ± 22.1 ED (mSv) 8.2 ± 5.3
BMI, body mass index; cCTA, coronary CT angiography; CTDlvol, computed tomography index volume; DLP, dose–length product; ED, effective dose.
Data are n (%) or mean ± standard deviation unless otherwise indicated.
Table 2
Agatston Calcium Scores and Extent of Coronary Artery Disease in This Patient Cohort
Calcium scores ∗ 0 20 (40) 1–10 3 (6) 11–100 2 (4) 101–400 9 (18) >400 10 (20) Vessel disease No vessel disease 21 (42) Single vessel 6 (12) Two vessel 6 (12) Three vessel 17 (34)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Image Analysis
Get Radiology Tree app to read full this article<
Table 3
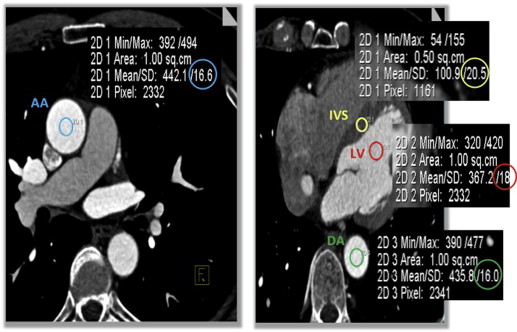
Image Noise and CT Attenuation in Four Anatomical Regions of Interest, the Ascending Aorta (AA), Descending Aorta (DA), Interventricular Septum (IVS), and Left Ventricle (LV), in IRIS and FBP Reconstructions
ROI Image Noise (HU) Attenuation (HU) FBP IRIS_t_ Value_P_ Value FBP IRIS_t_ Value_P_ Value AA 27.1 ± 8.9 20.8 ± 8.3 12.315 .001 ∗ 409.6 ± 77.7 406.5 ± 76.2 1.871 .067 DA 33.5 ± 13.5 23.3 ± 8.8 8.994 .001 ∗ 377.5 ± 73.7 376.5 ± 74.4 0.809 .422 IVS 30.6 ± 12.8 23.5 ± 9.6 7.233 .001 ∗ 111.0 ± 18.1 110.2 ± 19.1 0.664 .51 LV 32.9 ± 13.1 25.4 ± 10.6 6.035 .001 ∗ 361.2 ± 81.6 359.1 ± 81.9 1.059 .295
FBP, filtered back-projection; IRIS, iterative reconstruction in image space; ROI, region of interest.
Get Radiology Tree app to read full this article<
Table 4
Image Analysis and Coronary Segmentation Analysis
IRIS FBP_t_ Value_P_ Value Image noise (HU) 23.3 ± 8.1 31.0 ± 11.1 10.520 .0001 ∗ Image quality 3.2 ± 1.0 3.0 ± 1.0 2.137 .038 ∗ Time (sec) 95.2 ± 38.2 111.9 ± 40.5 3.117 .003 ∗ Manual adjustments 5.7 ± 3.0 6.8 ± 3.6 2.895 .006 ∗ Segments missing 3.6 ± 1.8 3.8 ± 1.9 1.269 .210
FBP, filtered back-projection; IRIS, iterative reconstruction in image space.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Coronary Segmentation Analysis
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Budoff M.J., Dowe D., Jollis J.G., et. al.: Diagnostic performance of 64-multidetector row coronary computed tomographic angiography for evaluation of coronary artery stenosis in individuals without known coronary artery disease: results from the prospective multicenter ACCURACY (Assessment by Coronary Computed Tomographic Angiography of Individuals Undergoing Invasive Coronary Angiography) trial. J Am Coll Cardiol 2008; 52: pp. 1724-1732.
2. Meijboom W.B., van Mieghem C.A., Mollet N.R., et. al.: 64-Slice computed tomography coronary angiography in patients with high, intermediate, or low pretest probability of significant coronary artery disease. J Am Coll Cardiol 2007; 50: pp. 1469-1475.
3. Brooks R.A., Di Chiro G.: Theory of image reconstruction in computed tomography. Radiology 1975; 117: pp. 561-572.
4. Wedegartner U., Yamamura J., Nagel H.D., et. al.: Image quality of thickened slabs in multislice CT chest examinations: postprocessing versus direct reconstruction. Rofo 2007; 179: pp. 373-379.
5. Matsumoto S., Ohno Y., Yamagata H., et. al.: Potential contribution of multiplanar reconstruction (MPR) to computer-aided detection of lung nodules on MDCT. Eur J Radiol 2012; 81: pp. 366-370.
6. Bashir M.R., Dale B.M., Merkle E.M., et. al.: Automated liver sampling using a gradient dual-echo Dixon-based technique. Magn Reson Med 2012; 67: pp. 1469-1477.
7. Tingelhoff K., Moral A.I., Kunkel M.E., et. al.: Comparison between manual and semi-automatic segmentation of nasal cavity and paranasal sinuses from CT images. Conf Proc IEEE Eng Med Biol Soc 2007; 2007: pp. 5505-5508.
8. Bittencourt M.S., Schmidt B., Seltmann M., et. al.: Iterative reconstruction in image space (IRIS) in cardiac computed tomography: initial experience. Int J Cardiovasc Imaging 2011; 27: pp. 1081-1087.
9. Moscariello A., Takx R.A., Schoepf U.J., et. al.: Coronary CT angiography: image quality, diagnostic accuracy, and potential for radiation dose reduction using a novel iterative image reconstruction technique-comparison with traditional filtered back projection. Eur Radiol 2011; 21: pp. 2130-2138.
10. Park E.A., Lee W., Kim K.W., et. al.: Iterative reconstruction of dual-source coronary CT angiography: assessment of image quality and radiation dose. Int J Cardiovasc Imaging 2012; 28: pp. 1775-1786.
11. Thibault J.B., Sauer K.D., Bouman C.A., et. al.: A three-dimensional statistical approach to improved image quality for multislice helical CT. Med Phys 2007; 34: pp. 4526-4544.
12. Willemink M.J., de Jong P.A., Leiner T., et. al.: Iterative reconstruction techniques for computed tomography, part 1: technical principles. Eur Radiol 2013; 23: pp. 1623-1631.
13. Beister M., Kolditz D., Kalender W.A.: Iterative reconstruction methods in X-ray CT. Phys Med 2012; 28: pp. 94-108.
14. Austen W.G., Edwards J.E., Frye R.L., et. al.: A reporting system on patients evaluated for coronary artery disease. Report of the Ad Hoc Committee for Grading of Coronary Artery Disease, Council on Cardiovascular Surgery, American Heart Association. Circulation 1975; 51: pp. 5-40.
15. Abdulla J., Abildstrom S.Z., Gotzsche O., et. al.: 64-Multislice detector computed tomography coronary angiography as potential alternative to conventional coronary angiography: a systematic review and meta-analysis. Eur Heart J 2007; 28: pp. 3042-3050.
16. Budoff M.J., Achenbach S., Blumenthal R.S., et. al.: Assessment of coronary artery disease by cardiac computed tomography: a scientific statement from the American Heart Association Committee on Cardiovascular Imaging and Intervention, Council on Cardiovascular Radiology and Intervention, and Committee on Cardiac Imaging, Council on Clinical Cardiology. Circulation 2006; 114: pp. 1761-1791.
17. Hamon M., Biondi-Zoccai G.G., Malagutti P., et. al.: Diagnostic performance of multislice spiral computed tomography of coronary arteries as compared with conventional invasive coronary angiography: a meta-analysis. J Am Coll Cardiol 2006; 48: pp. 1896-1910.
18. Johnson T.R., Nikolaou K., Busch S., et. al.: Diagnostic accuracy of dual-source computed tomography in the diagnosis of coronary artery disease. Invest Radiol 2007; 42: pp. 684-691.
19. Rist C., Johnson T.R., Muller-Starck J., et. al.: Noninvasive coronary angiography using dual-source computed tomography in patients with atrial fibrillation. Invest Radiol 2009; 44: pp. 159-167.
20. Babin D., Vansteenkiste E., Pizurica A., et. al.: Segmentation of brain blood vessels using projections in 3-D CT angiography images. Conf Proc IEEE Eng Med Biol Soc 2011; 2011: pp. 8475-8478.
21. Biesdorf A., Rohr K., Feng D., et. al.: Segmentation and quantification of the aortic arch using joint 3D model-based segmentation and elastic image registration. Med Image Anal 2012; 16: pp. 1187-1201.
22. Lesage D., Angelini E.D., Bloch I., et. al.: Bayesian maximal paths for coronary artery segmentation from 3D CT angiograms. Med Image Comput Comput Assist Interv 2009; 12: pp. 222-229.
23. Zheng Y., Tek H., Funka-Lea G., et. al.: Efficient detection of native and bypass coronary ostia in cardiac CT volumes: anatomical versus pathological structures. Med Image Comput Comput Assist Interv 2011; 14: pp. 403-410.