
Rationale and Objectives
To determine the incidence of breast cancer in women presenting for fine needle aspiration of sonographically diagnosed complicated breast cysts.
Materials and Methods
Institutional review board approval was obtained. A retrospective study was performed of 186 consecutive women who presented for fine needle aspiration of 243 sonographic complicated cysts detected by clinical examination or imaging between January 2002 and August 2003. Sonographic complicated cysts were defined as those meeting most but not all criteria for simple cysts similar to current Breast Imaging Reporting and Data System classification. We excluded solid masses, cysts with solid components, intracystic masses, and simple cysts. Prospective mammography, ultrasound, and procedure reports were reviewed. A case was considered positive if cytology, core needle biopsy, or surgical excision was positive for cancer. Final diagnosis was established by biopsy, cytology, clinical resolution, or stability over time.
Results
One of 243 (0.4%) lesions proved malignant (95% confidence interval 0–1.94%); 210/243 (86.4%) of cases yielded fluid on aspiration. Of 141 samples submitted to cytology, 138 (97.9%) were benign and 3 (2.1%) atypical. All cases of atypia were benign at surgical excision. Ninety five of 243 (39.1%) aspiration samples with typical cyst fluid were discarded. A total of 33/243 (13.6%) cases did not yield fluid, 1 of which was positive for cancer. Thirty cases underwent core needle or excisional biopsy for imaging discordance with benign results.
Conclusions
Breast cancer presenting as a complicated cyst by ultrasound was rare (0.4%, 95% confidence interval 0–1.94%). These results provide support for classification of complicated cysts as probably benign.
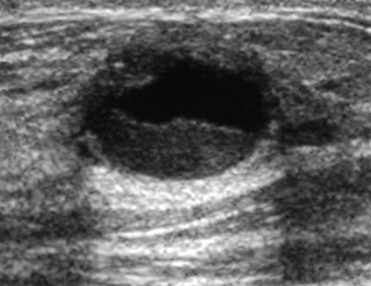
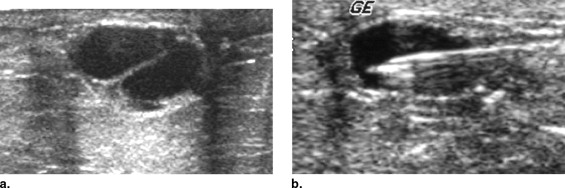
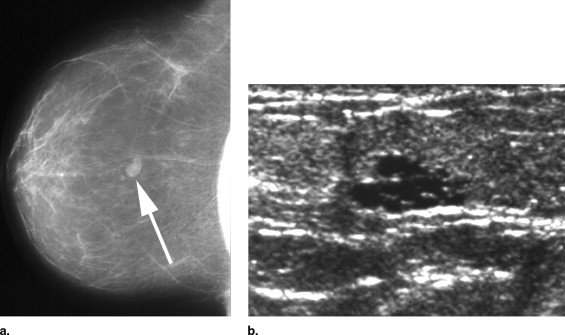
Breast sonography is widely accepted as an excellent tool to further characterize masses detected by mammography or physical examination and plan for biopsy. Characterization of solid and cystic masses represents a critical point in the workup of breast abnormalities. Cysts are a nearly ubiquitous breast condition and are usually benign; however, malignancy does rarely occur ( ). Simple cysts as described in the current ultrasound (US) Breast Imaging Reporting and Data System (BI-RADS) lexicon ( ) (circumscribed, anechoic, posterior acoustic enhancement, lack of Doppler signal, and absence of solid components) are by definition benign; no intervention is necessary ( ). Those that are not simple may contain homogeneous or heterogeneous internal echoes, perceptible walls, septations, debris, lack posterior acoustic enhancement, or be composed of clustered microcysts. The US BI-RADS lexicon now separates non-simple cysts into complicated cysts (the subject of this investigation) and complex masses. It is generally accepted that those lesions classified as complex masses with mixed cystic and solid components or an intracystic solid mass should be referred for core or excisional biopsy ( ). Management of complicated cysts is less uniform.
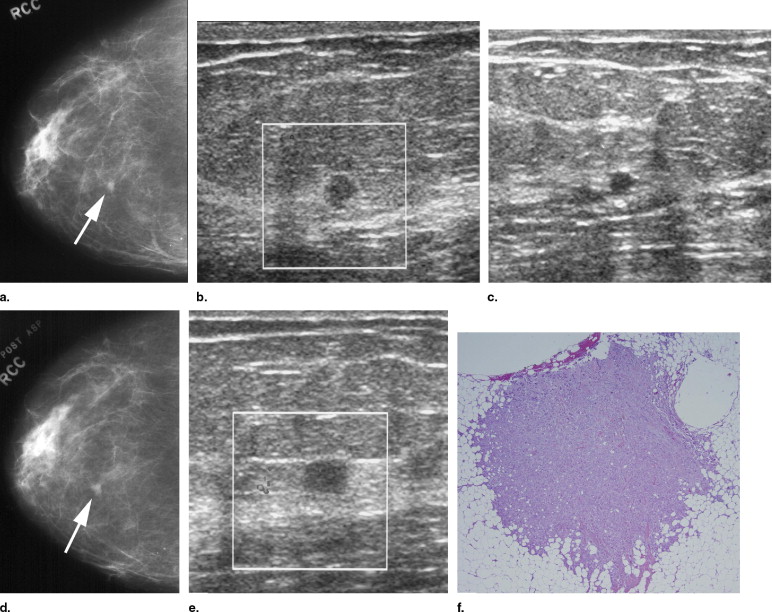
Controversy remains in the radiology and surgical literature regarding the appropriate management of complicated cysts demonstrating most but not all features of simple cysts. Fine needle aspiration (FNA) provides an easy means for evaluating complicated cysts and may determine whether a mass is cystic or solid and assess the nature of cyst contents. If using sonography, FNA may also determine whether the mass has resolved as a result of the procedure. National Comprehensive Cancer Network guidelines recommend aspiration of symptomatic or non-simple palpable cysts ( ). Previous authors ( ) have investigated the rate of malignancy in complicated cysts and found cancer to be uncommon, suggesting that intervention may not be necessary. However, these studies were limited by small sample size, case selection, and incomplete follow-up.
Get Radiology Tree app to read full this article<
Material and methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
References
1. Reuter K., D’Orsi C.J., Reale F.: Intracystic carcinoma of the breast: the role of ultrasonography. Radiology 1984; 153: pp. 233-234.
2. Dogan B.E., Whitman G.J., Middleton L.P., et. al.: Intracystic papillary carcinoma of the breast. AJR Am J Roentgenol 2003; 181: pp. 186.
3. Obenauer S., Dammert S.: Palpable masses in breast during lactation. Clin Imaging 2007; 31: pp. 1-5.
4. American College of Radiology: Breast imaging reporting and data system (BI-RADS).3rd ed.2003.American College of RadiologyReston, VA
5. Bassett L.W., Kimme-Smith C.: Breast sonography. AJR Am J Roentgenol 1991; 156: pp. 449-455.
6. Berg W.A., Campassi C.I., Ioffe O.B.: Cystic lesions of the breast: sonographic-pathologic correlation. Radiology 2003; 227: pp. 183-191.
7. Houssami N., Irwig L., Ung O.: Review of complex breast cysts: implications for cancer detection and clinical practice. ANZ J Surg 2005; 75: pp. 1080-1085.
8. Vargas H.I., Vargas M.P., Gonzalez K.D., et. al.: Outcomes of sonography-based management of breast cysts. Am J Surg 2004; 188: pp. 443-447.
9. The Breast Cancer Screening and Diagnoses Clinical Practice Guidelines in Oncology (version v.1.2005). http://www.nccn.org Accessed on December 1, 2006
10. Venta L.A., Kim J.P., Pelloski C.E., et. al.: Management of complex breast cysts. Am J Roentgenol 1999; 173: pp. 1331-1336.
11. Buchberger W., DeKoekkoek-Doll P., Springer P., et. al.: Incidental findings on sonography of the breast: clinical significance and diagnostic workup. AJR Am J Roentgenol 1999; 173: pp. 921-927.
12. Louie L., Velez N., Earnest D., et. al.: Management of nonpalpable ultrasound-indeterminate breast lesions. Surgery 2003; 134: pp. 667-673.
13. Smith D.N., Kaelin C.M., Korbin C.D., et. al.: Impalpable breast cysts: utility of cytologic examination of fluid obtained with radiologically guided aspiration. Radiology 1997; 204: pp. 149-151.
14. Ihaka R., Gentleman R.: A Language and Environment for Statistical Computing.2004.The R Development Core TeamVienna
15. Stavros A.T., Thickman D., Rapp C.L., et. al.: Solid breast nodules: use of sonography to distinguish between benign and malignant lesions. Radiology 1995; 196: pp. 123-134.
16. Graf O., Helbich T.H., Hopf G., et. al.: Probably benign breast masses at US: is follow-up an acceptable alternative to biopsy?. Radiology 2007; 244: pp. 87-93.
17. Hilton S.V., Leopold G.R., Olson L.K., et. al.: Real-time breast sonography: application in 300 consecutive patients. Am J Roentgenol 1986; 147: pp. 479-486.
18. Pisano E.D., Fajardo L.L., Caudry D.J., et. al.: Fine-needle aspiration biopsy of nonpalpable breast lesions in a multicenter clinical trial: results from the Radiologic Diagnostic Oncology Group V. Radiology 2001; 219: pp. 785-792.
19. Omori L., Hisa N., Ohkuma K., et. al.: Breast masses with mixed cystic-solid sonographic appearance. J Clin Ultrasound 1993; 21: pp. 489-495.
20. Rahbar G., Sie A.C., Hansen G.C., et. al.: Benign versus malignant solid breast masses: US differentiation. Radiology 1999; 213: pp. 889-894.
21. Berg W.A.: Sonographically depicted breast clustered microcysts: is follow-up appropriate?. AJR Am J Roentgenol 2005; 185: pp. 952-959.