
Rationale and Objective
The aim of this study was to evaluate the uncertainty in computed tomographic pulmonary angiography (CTPA) radiology reports, manifested by descriptions of report limitations and image quality.
Materials and methods
CTPA reports between 2004 and 2006 were reviewed for patient demographic data (age, gender, pregnancy state), radiologist data (years of experience, subspecialty, final dictation by an attending radiologist vs a resident being present and dictating the report), the presence of pulmonary embolism (PE), and key words describing examination quality and limitations.
Results
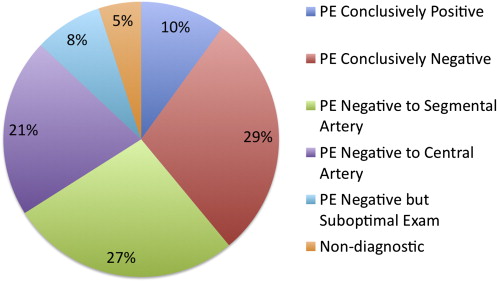
There were 2151 CTPA reports. Patterns of reporting CTPA in the impression sections of radiology reports were as follows: (1) PE conclusively positive (10%), (2) PE conclusively negative (29%), (3) PE negative to segmental arteries (27%), (4) PE negative to central pulmonary arteries (21%), (5) PE negative but suboptimal examination (8%), and (6) nondiagnostic examination (5%). Among the last three categories, seven PEs were not initially diagnosed but were found on subsequent imaging examinations. Limitations in image quality, respiratory motion artifact, and contrast enhancement were most frequently mentioned as limitations in image quality (62% and 28% of all reports, respectively). Radiologists tended to report limitations in image quality if they were thoracic radiology subspecialists, had >10 years of experience, or worked independently ( P < .001).
Conclusion
Different patterns of reporting CTPA exist and vary on the basis of individual radiologists’ subspecialties, experience, and whether they work independently or with residents. Certain wording regarding the presence of PE may falsely imply negativity of PE in a limited examination.
The radiology report is the final document that describes the findings of a radiologic consultation by a radiologist and is forwarded to the referring physician. Most of the images are not viewed by the referring physician, and as a result, the referring physician depends highly on the radiology report for diagnosing the patient’s condition. The American College of Radiology has provided guidelines for the communication of diagnostic imaging findings, with a detailed section describing what constitutes an official radiology report , but adherence to the guidelines by the radiology community is not known. With availability of picture archiving and communication system and teleradiology, radiologists have decreased contact with referring physicians. Thus, the importance of the radiology report is even more significant.
In a large institution where there are many radiologists, the variation in reports of the same type of examination can be wide, from the number of words the authors use to describe the same findings, to differences in vocabulary, to the manner in which the reports are structured . These variations can contribute to a lack of uniformity and quality. The variation across different radiologists can also be a source of frustration for referring physicians. Cohesive, clear reports with less variation in style and content can help referring physicians improve the quality of care they provide to their patients. Therefore, a meaningful radiology report needs to be concise, unambiguous, and clearly answer the clinical questions.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Study Design
Get Radiology Tree app to read full this article<
Study Setting and Population
Get Radiology Tree app to read full this article<
Study Protocol
Get Radiology Tree app to read full this article<
Measurement, Data Collection, and Processing
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Outcome Measures
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Examination Population, Pattern Of Reporting The Presence Of PE, And Quality Of Studies
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Frequencies of Factors Reported as Limiting Interpretation of Computed Tomographic Pulmonary Angiographic Examinations ( n = 2151)
Factor Number (Examinations) Percentage Patient-related factors Respiratory motion 1340 62.3 Image noise and body habitus 134 6.2 Lung and pleural abnormalities 65 3.0 Cardiac motion 10 0.5 Flow-related artifact 8 0.4 Technical factors Suboptimal contrast opacification 596 27.7 Streak, beam-hardening artifacts 70 3.3 Gantry-related artifact 1 0.05 Gadolinium contrast use 1 0.05 Unspecified technical factors 29 1.3 Not specified 106 4.9
Percentages Are Not Mutually Exclusive.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Factors Associated with the Presence of Limitations Dictated in Radiology Reports
Factor Distribution (Number of Reports) Limitations P Patient’s age (y) ≤60 1146 1058 (92.3%) .013 >60 1005 896 (89.2%) Patient’s gender Male 1070 969 (90.6%) .654 Female 1081 985 (91.1%) Pregnancy Yes 14 14 (100%) .288 No 1067 985 (91.1%) Radiologists’ subspecialty Thoracic radiologists ( n = 11) 791 791 (100%) <.001 Nonthoracic radiologists ( n = 60) 1360 1163 (85.5%) Radiologists’ experience (y) ≤10 1069 939 (87.8%) <.001 >10 1082 1015 (93.8%) Radiologist interpretation Resident being present and dictating the report 1745 1567 (89.8%) <.001 Final dictation by an attending radiologist 406 387 (95.3%)
Table 3
Two-by-Two Table Demonstrating the Effect of Limitations on Reporting Patterns of Computed Tomographic Pulmonary Angiography
Limitation Statement in Report Conclusive Diagnosis of PE ∗ Inconclusive Diagnosis of PE † Total Reports Absent 196 1 197 Present 1209 745 1954 Total reports 1405 746 2151
PE, pulmonary embolism.
Fisher’s exact test, two-tailed P < .0001.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Follow-Up Imaging Examinations
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Limitations
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
References
1. The American College of Radiology. ACR practice guideline for communication of diagnostic imaging findings (revision 2005). Available at: http://www.acr.org/SecondaryMainMenuCategories%2fquality_safety%2fguidelines%2fdx%2fcomm_diag_rad.aspx . Accessed November 6, 2008.
2. Khorasani R., Bates D.W., Teeger S., Rothschild J.M., Adams D.F., Seltzer S.E.: Is terminology used effectively to convey diagnostic certainty in radiology reports?. Acad Radiol 2003; 10: pp. 685-688.
3. DeMonaco N.A., Dang Q., Kapoor W.N., Ragni M.V.: Pulmonary embolism incidence is increasing with use of spiral computed tomography. Am J Med 2008; 121: pp. 611-617.
4. Donohoo J.H., Mayo-Smith W.W., Pezzullo J.A., Egglin T.K.: Utilization patterns and diagnostic yield of 3421 consecutive multidetector row computed tomography pulmonary angiograms in a busy emergency department. J Comput Assist Tomogr 2008; 32: pp. 421-425.
5. Glassroth J.: Imaging of pulmonary embolism. JAMA 2007; 298: pp. 2788-2789.
6. Tapson V.F.: Acute pulmonary embolism. N Engl J Med 2008; 358: pp. 1037-1052.
7. Patel S., Kazerooni E.A., Cascade P.N.: Pulmonary embolism: optimization of small pulmonary artery visualization at multi-detector row CT. Radiology 2003; 227: pp. 445-460.
8. Brunot S., Corneloup O., Latrabe V., Montaudon M., Laurent F.: Reproducibility of multi-detector spiral computed tomography in detection of sub-segmental acute pulmonary embolism. Eur Radiol 2005; 15: pp. 2057-2063.
9. Anderson D.R., Kahn S.R., Rodger M.A., et. al.: Computed tomographic pulmonary angiography vs ventilation-perfusion lung scanning in patients with suspected pulmonary embolism: a randomized controlled trial. JAMA 2007; 298: pp. 2743-2753.
10. Quiroz R., Kucher N., Zou K.H., et. al.: Clinical validity of a negative computed tomography scan in patients with suspected pulmonary embolism. JAMA 2005; 293: pp. 2012-2017.
11. Garg K., Sieler H., Welsh C.H., Johnston R.J., Russ P.D.: Clinical validity of helical CT being interpreted as negative for pulmonary embolism: implications for patient treatment. AJR Am J Roentgenol 1999; 172: pp. 1627-1631.
12. Lomis N.N., Yoon H.C., Moran A.G., Miller F.J.: Clinical outcomes of patients after a negative spiral CT pulmonary arteriogram in the evaluation of acute pulmonary embolism. J Vasc Interv Radiol 1999; 10: pp. 707-712.
13. Winer-Muram H.T., Rydberg J., Johnson M.S., et. al.: Suspected acute pulmonary embolism: evaluation with multi-detector row CT versus digital subtraction pulmonary arteriography. Radiology 2004; 233: pp. 806-815.
14. Coche E., Verschuren F., Keyeux A., et. al.: Diagnosis of acute pulmonary embolism in outpatients: comparison of thin-collimation multi-detector row spiral CT and planar ventilation-perfusion scintigraphy [published correction appears in Radiology 2004; 232:627–628]. Radiology 2003; 229: pp. 757-765.
15. Blachere H., Latrabe V., Montaudon M., et. al.: Pulmonary embolism revealed on helical CT angiography: comparison with ventilation-perfusion radionuclide lung scanning. AJR Am J Roentgenol 2000; 174: pp. 1041-1047.
16. Gottsäter A., Berg A., Centergård J., Frennby B., Nirhov N., Nyman U.: Clinically suspected pulmonary embolism: is it safe to withhold anticoagulation after a negative spiral CT?. Eur Radiol 2001; 11: pp. 65-72.
17. Ost D., Rozenshtein A., Saffran L., Snider A.: The negative predictive value of spiral computed tomography for the diagnosis of pulmonary embolism in patients with nondiagnostic ventilation-perfusion scans. Am J Med 2001; 110: pp. 16-21.
18. Nilsson T., Olausson A., Johnsson H., Nyman U., Aspelin P.: Negative spiral CT in acute pulmonary embolism. Acta Radiol 2002; 43: pp. 486-491.
19. Donato A.A., Scheirer J.J., Atwell M.S., Gramp J., Duszak R.: Clinical outcomes in patients with suspected acute pulmonary embolism and negative helical computed tomographic results in whom anticoagulation was withheld. Arch Intern Med 2003; 163: pp. 2033-2038.
20. Krestan C.R., Klein N., Fleischmann D., et. al.: Value of negative spiral CT angiography in patients with suspected acute PE: analysis of PE occurrence and outcome. Eur Radiol 2004; 14: pp. 93-98.
21. Remy-Jardin M., Mastora I., Remy J.: Pulmonary embolus imaging with multislice CT. Radiol Clin N Am 2003; 41: pp. 507-519.
22. Stein P.D., Woodard P.K., Weg J.G., et. al.: Diagnostic pathways in acute pulmonary embolism: recommendations of the PIOPED II investigators. Radiology 2007; 242: pp. 15-21.
23. Remy-Jardin M., Pistolesi M., Goodman L.R., et. al.: Management of suspected acute pulmonary embolism in the era of CT angiography: a statement from the Fleischner Society. Radiology 2007; 245: pp. 315-329.
24. Wittram C.: How I do it: CT pulmonary angiography. AJR Am J Roentgenol 2007; 188: pp. 1255-1261.
25. Moores L.K., Jackson W.L., Shorr A.F., Jackson J.L.: Meta-analysis: outcomes in patients with suspected pulmonary embolism managed with computed tomographic pulmonary angiography. Ann Intern Med 2004; 141: pp. 866-874.
26. Remy-Jardin M., Remy J., Baghaie F., Fribourg M., Artaud D., Duhamel A.: Clinical value of thin collimation in the diagnostic workup of pulmonary embolism. AJR Am J Roentgenol 2000; 175: pp. 407-411.
27. Lorut C., Ghossains M., Horellou M.H., Achkar A., Fretault J., Laaban J.P.: A noninvasive diagnostic strategy including spiral computed tomography in patints with suspected pulmonary embolism. Am J Respir Crit Care Med 2000; 162: pp. 1413-1418.
28. Perrier A., Howarth N., Didier D., et. al.: Performance of helical computed tomography in unselected outpatients with suspected pulmonary embolism. Ann Intern Med 2001; 135: pp. 88-97.
29. Musset D., Parent F., Meyer G., et. al.: Diagnostic strategy for patients with suspected pulmonary embolism: a prospective multicentre outcome study. Lancet 2002; 360: pp. 1914-1920.
30. Remy-Jardin M., Tillie-Leblond I., Szapiro D., et. al.: CT angiography of pulmonary embolism in patients with underlying respiratory disease: impact of multislice CT on image quality and negative predictive value. Eur Radiol 2002; 12: pp. 1971-1978.
31. Tillie-Leblond I., Mastora I., Radenne F., et. al.: Risk of pulmonary embolism after a negative spiral CT angiogram in patients with pulmonary disease: 1-year clinical follow-up study. Radiology 2002; 223: pp. 461-467.
32. van Strijen M.J., de Monyé W., Schiereck J., et. al.: Single-detector helical computed tomography as the primary diagnostic test in suspected pulmonary embolism: a multicenter clinical management study of 510 patients. Ann Intern Med 2003; 138: pp. 307-314.
33. Stein P.D., Fowler S.E., Goodman L.R., et. al.: Multidetector computed tomography for acute pulmonary embolism. N Engl J Med 2006; 354: pp. 2317-2327.
34. Perrier A., Roy P., Sanchez O., et. al.: Multidetector-row computed tomography in suspected pulmonary embolism. N Engl J Med 2005; 352: pp. 1760-1768.
35. Perrier A., Roy P., Aujesky D., et. al.: Diagnosing pulmonary embolism in outpatients with clinical assessment, d-dimer measurement, venous ultrasound, and helical computed tomography: a multicenter management study. Am J Med 2004; 116: pp. 291-299.
36. Arakawa H., Kohno T., Hiki T., Kaji Y.: CT pulmonary angiography and CT venography: factors associated with vessel enhancement. AJR Am J Roentgenol 2007; 189: pp. 156-161.