
Rationale and Objectives
To evaluate the performance of a computer-aided detection (CAD) system with bone suppression imaging when applied to unselected consecutive chest radiographs (CXRs) with computed tomography (CT) correlation.
Materials and Methods
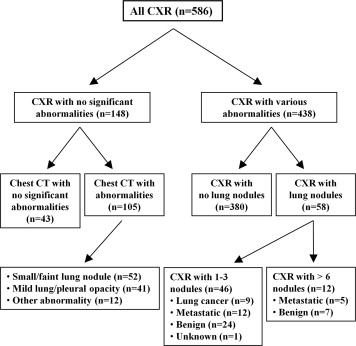
This study included 586 consecutive patients with standard or portable CXRs who had a chest CT scan on the same day. Among the 586 CXRs, 438 had various abnormalities, including 46 CXRs with 66 lung nodules, and 148 CXRs had no significant abnormalities. A commercially available CAD system was applied to all 586 CXRs. True nodules and false positives (FPs) marked on CXRs by the CAD system were evaluated based on the corresponding chest CT findings.
Results
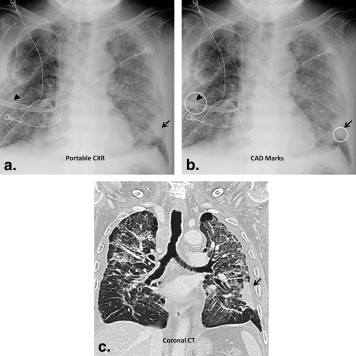
The CAD system marked 47 of 66 (71%) lung nodules in this consecutive series of CXRs. The mean FP rate per image was 1.3 across all 586 CXRs, with 1.5 FPs per image on the 438 abnormal CXRs and 0.8 FPs per image on the 148 normal CXRs. A total of 41% of the 752 FP marks were related to non-nodule pathologic findings.
Conclusions
A currently available CAD system marked 71% of radiologist-identified lung nodules in a large consecutive series of CXRs, and 41% of “false” marks were caused by pathologic findings.
Potentially resectable lung cancers missed by radiologists on conventional chest radiographs (CXRs) in clinical practice are mostly located in the lung periphery and have a median diameter of about 20 mm . Even under the constrained conditions of an observer performance study, where observers are specifically focused on nodule detection, about 40% of all subtle cancers remain undetected by radiologists . However, advances in radiographic chest imaging such as dual–energy subtraction (DES), temporal subtraction, and computer-aided detection (CAD) have the potential to improve radiologists’ performance in the detection of subtle, obscured, or otherwise potentially overlooked lung cancers .
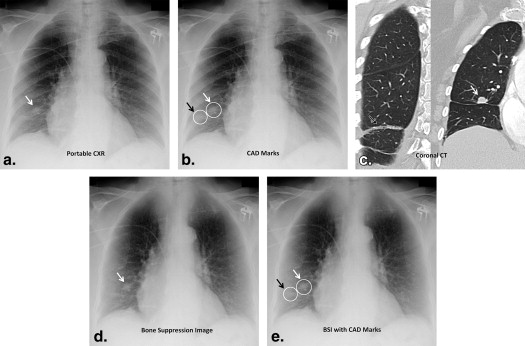
Previous reports of a Food and Drug Administration–approved chest CAD system (OnGuard, Riverain Medical) applied to the detection of radiologist-missed lung cancers on CXRs described relatively low sensitivity and a high number of false-positive (FP) detections (35% sensitivity with 5.9 FPs per radiograph with OnGuard 1.0 and 50% sensitivity with 3.9 FPs per radiograph with OnGuard 3.0 ). Over the past few years, however, newer versions of the same nodule detection system have achieved higher lung nodule detection sensitivities with markedly improved specificity compared to these earlier versions . This CAD system recently incorporated bone suppression imaging (BSI) , which, in addition to impacting CAD system performance, can improve radiologists’ accuracy in the detection of lung nodules and discrimination between true-positive and FP CAD marks on CXRs through direct visualization of the BSI images.
Get Radiology Tree app to read full this article<
Materials and methods
Chest Radiographs and Chest CT Scans
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
CAD System
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Data Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Imaging Findings on Chest Radiographs and Chest CT Scans
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
CAD Performance Compared to Imaging Findings
Get Radiology Tree app to read full this article<
Table 1
CAD Detection Rates on the 46 CXRs with One to Three Nodules (Total of 66 Nodules)
Group No. of Nodules No. of Nodules Marked by CAD CAD Detection Rate (%) CXR-based nodule size, mm 5–10 13 4 31 10–20 30 23 77 20–30 23 20 87 Subtlety 1–3 (very subtle) 38 19 50 4–6 (relatively subtle) 24 24 100 7–9 (obvious) 4 4 100 All nodules 66 47 71
CAD, computer-aided detection; CXR, chest radiograph.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
CAD False-Positive Findings on 586 CXRs
Group No. of CXRs No. of FPs FP Rate ∗ (FP/CXR) FPs Due to Anatomic Structure, n (%) FPs Due to Pathologic Change, n (%) FPs Due to Medical Device, n (%) CXR procedure Erect PA 248 266 1.1 ± 1.1 135 (51) 116 (44) 15 (6) Portable AP 338 486 1.4 ± 1.2 166 (34) 195 (40) 125 (26) Imaging finding No significant abnormality 148 117 0.8 ± 0.9 92 (79) 7 (6) 18 (15) With abnormal findings 438 635 1.5 ± 1.2 209 (33) 302 (48) 122 (19) <50% of lung area 226 264 1.2 ± 1.1 117 (45) 99 (37) 48 (18) ≥50% of lung area 212 371 1.8 ± 1.2 92 (25) 205 (55) 74 (20) All groups 586 752 1.3 ± 1.2 301 (40) 311 (41) 140 (19)
AP, anteroposterior; CAD, computer-aided detection; CXR, chest radiograph; FP, false positive; PA, posteroanterior.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
References
1. Shah P.K., Austin J.H.M., White C.S., et. al.: Missed non-small cell lung cancers: radiographic findings of potentially resectable lesions evident only in retrospect. Radiology 2003; 226: pp. 235-241.
2. Monnier-Cholley L., Carrat F., Cholley B.P., et. al.: Detection of lung cancer on radiographs: receiver operating characteristic analysis of radiologists’, pulmonologists’ and anesthesiologists’ performance. Radiology 2004; 33: pp. 799-805.
3. McAdams H.P., Samei E., Dobbins J., et. al.: Recent advances in chest radiography. Radiology 2006; 241: pp. 663-683.
4. MacMahon H., Li F., Engelmann R., et. al.: Dual energy subtraction and temporal subtraction chest radiography. J Thorac Imaging 2008; 23: pp. 77-85.
5. De Boo D.W., Prokop M., Uffmann M., et. al.: Computer-aided detection (CAD) of lung nodules and small tumours on chest radiographs. Eur J Radiol 2009; 72: pp. 218-225.
6. Li F., Engelmann R., Metz C.E., et. al.: Lung cancers missed on chest radiographs: results obtained with a commercial computer-aided detection program. Radiology 2008; 246: pp. 273-280.
7. White C.S., Flukinger T., Jeudy J., et. al.: Use of a computer-aided detection system to detect missed lung cancers at chest radiography. Radiology 2009; 252: pp. 273-281.
8. Meziane M., Mazzone P., Novak E., et. al.: A comparison of four versions of a computer-aided detection system for pulmonary nodules on chest radiographs. J Thorac Imaging 2012; 27: pp. 58-64.
9. Freedman M.T., Benedict Lo S.C., Seibel J.C., et. al.: Lung nodules: improved detection with software that suppresses the rib and clavicle on chest radiographs. Radiology 2011; 260: pp. 265-273.
10. Li F., Hara T., Shiraishi J., et. al.: Improved detection of subtle lung nodules by use of chest radiographs with bone suppression imaging: receiver operating characteristic analysis with and without localization. AJR Am J Roentgenol 2011; 196: pp. W535-W541.
11. Li F., Engelmann R., Pesce L., et. al.: Small lung cancers: improved detection by use of bone suppression imaging—comparison with dual-energy subtraction chest radiographs. Radiology 2011; 261: pp. 937-949.
12. Szucs-Farkas Z., Schick A., Cullmann J.L., et. al.: Comparison of dual-energy subtraction and electronic bone suppression combined with computer-aided detection on chest radiographs: effect on human observers’ performance in nodule detection. AJR Am J Roentgenol 2013; 200: pp. 1006-1013.
13. Schalekamp S., van Ginneken B., Koedam E., et. al.: Computer-aided detection improves detection of pulmonary nodules in chest radiographs beyond the support by bone-suppressed images. Radiology 2014; 272: pp. 252-261.
14. Henschke C.I., Yankelevitz D.F., Naldlch D.P., et. al.: CT screening for lung cancer: suspiciousness of nodules according to size on baseline scans. Radiology 2004; 231: pp. 164-168.
15. Freer T.W., Ulissey M.J.: Screening mammography with computer-aided detection: prospective study of 12,860 patients in a community breast center. Radiology 2001; 220: pp. 781-786.
16. Ellis R., Meade A., Mathiason M.A., et. al.: Evaluation of computer-aided detection system in the detection of small invasive breast carcinoma. Radiology 2007; 245: pp. 88-94.
17. Kim J.S., Moon W.K., Cho N., et. al.: Computer-aided detection in full-field digital mammography: sensitivity and reproducibility in serial examinations. Radiology 2008; 246: pp. 71-80.
18. Suzuki K., Abe H., MacMahon H., et. al.: Image-processing technique for suppressing ribs in chest radiographs by means of massive training artificial neural network (MTANN). IEEE Trans Med Imaging 2006; 25: pp. 406-416.
19. Loog M., van Ginneken B., Schilham A.M.R.: Filter learning: application to suppression of bony structures from chest radiographs. Med Image Anal 2006; 10: pp. 826-840.
20. Li F., Engelmann R., Pesce L., et. al.: Improved detection of focal pneumonia by chest radiography with bone suppression imaging. Eur Radiol 2012; 12: pp. 2729-2735.
21. Balkman J.D., Mehandru S., DuPont E., et. al.: Dual energy subtraction digital radiography improves performance of a next generation computer-aided detection program. J Thorac Imaging 2010; 25: pp. 41-47.
22. MacMahon H., Engelmann R., Behlen F.M., et. al.: Computer-aided diagnosis of pulmonary nodules: results of a large-scale observer test. Radiology 1999; 213: pp. 723-726.