
Rationale and Objectives
To describe the rationale, design, and technical background of coronary artery calcium (CAC) imaging in the large-scale population-based cardiovascular disease screening trial (Risk Or Benefit IN Screening for CArdiovascular Diseases [ROBINSCA]).
Materials and Methods
First, literature search was performed to review the logistics, setup, and settings of previously performed CAC imaging studies, and current clinical CAC imaging protocols of participating centers in the ROBINSCA trial were evaluated. A second literature search was performed to evaluate the impact of computed tomography parameter settings on CAC score.
Results
Based on literature reviews and experts opinion an imaging protocol accompanied by data management protocol was created for ROBINSCA. The imaging protocol should consist of a fixed tube voltage, individually tailored tube current setting, mid-diastolic electrocardiography-triggering, fixed field-of-view, fixed reconstruction kernel, fixed slice thickness, overlapping reconstruction and without iterative reconstruction. The analysis of scans is performed with one type and version of CAC scoring software, by two dedicated and experienced researchers. The data management protocol describes the organization of data handling between the coordinating center, participating centers, and core analysis center.
Conclusion
In this paper we describe the rationale and technical considerations to be taken in developing CAC imaging protocol, and we present a detailed protocol that can be implemented for CAC screening purposes.
Introduction
Early detection of cardiovascular disease (CVD) followed by evidence-based treatment could potentially reduce CVD morbidity and mortality . Extent of coronary artery calcium (CAC) is a strong risk marker for coronary events, with evidence mainly derived from observational studies and from prospective nonrandomized studies . So far, there is no evidence that CAC imaging followed by treatment leads to a decrease in CVD morbidity and mortality as prospective randomized studies on CVD risk stratification based on CAC imaging combined with treatment are lacking. Consequently, European and North-American guidelines on CVD prevention still classify the evidence for CAC imaging at level IIb (“may be considered”) in asymptomatic adults at intermediate risk and mention that CAC imaging should not be uncritically used as a screening method . However, there is an ongoing debate on whether and how a randomized controlled trial (RCT) to determine the risk or benefit of screening for CVD by CAC imaging should be performed . Issues related to RCT in CVD screening by CAC imaging, regarding radiation safety, imaging protocols, and privacy, and ethical and economic considerations, have been addressed by many experts in the field of CAC imaging . A well-described study design is essential when performing an RCT in CVD screening by CAC imaging. Moreover, in the case of such a trial, CAC imaging will most likely be performed in multiple centers involving many operators, technicians, and analysts. To use the CAC score as a quantitative imaging biomarker in a trial, the CAC score needs to be accurate, consistent, reliable, and valid across computed tomography (CT) platforms, clinical sites, and over time , demanding development of a robust and well-fitted imaging protocol.
In this paper we describe the rationale, design, and technical background of CAC imaging within the framework of the Dutch large-scale population-based cardiovascular screening trial, ROBINSCA (Risk Or Benefit IN Screening for CArdiovascular Diseases).
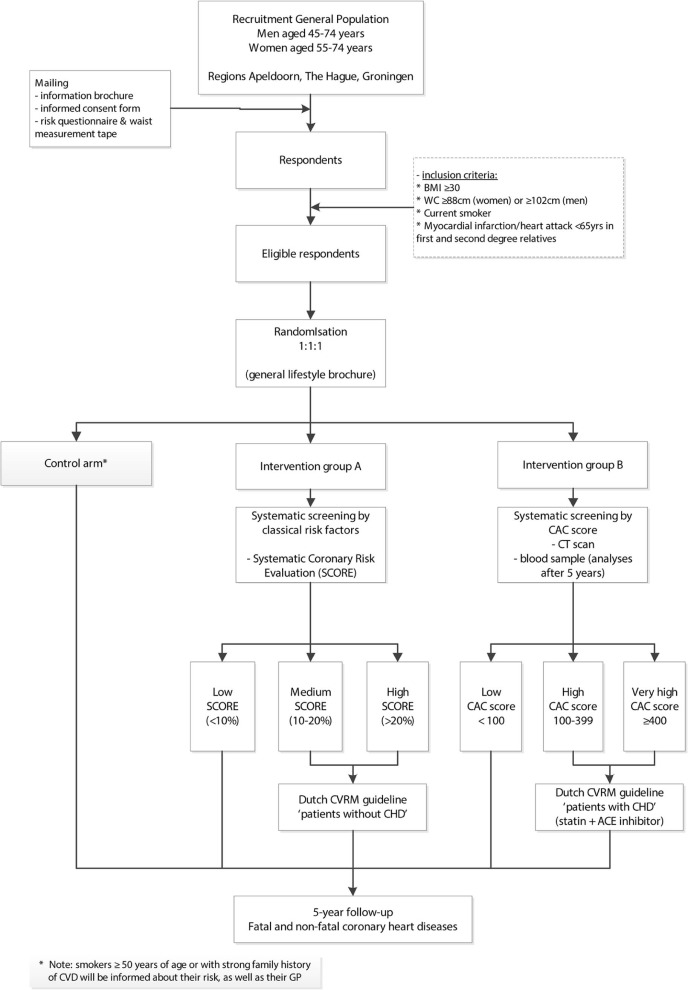
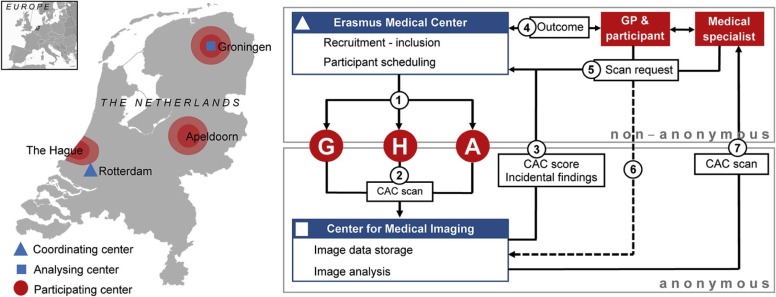
The ROBINSCA Trial
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and Methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Imaging Protocols in Previous CAC Studies
Get Radiology Tree app to read full this article<
TABLE 1
Coronary Artery Calcium Imaging Studies and their Protocol Settings
Study Author Year N Scanner Type ECG Triggering Scan Mode Tube Voltage Tube Current Recon Analysis St. Francis Heart Study Arad et al. 2000 1238 EBCT (Imatron C-150XP) 80% R-R interval 100 ms/Slice — — 3.0 mm (Contiguous), FOV 35 cm Threshold: 130 HU ≥2 adjacent pixels (≥0.93 mm 2 ) Arad et al. 2001 5582 EBCT (Imatron C-150XP) 80% R-R interval 100 ms/Slice — — 3.0 mm (Contiguous), FOV 26 cm, pixel area 0.51 mm 2 Threshold: 130 HU ≥2 adjacent pixels CARDIA study Iribarren et al. 2000 374 EBCT ECG gated Scantime: 100 ms — — 3.0 mm ≥6 Adjacent pixels (≥2 mm 2 ) Carr et al. 2005 3044 See MESA Pro and retrospective
80% R-R interval — — Yan et al. 2006 2913 EBCT, MDCT — 2 Sequential scans — — 2.5–3.0 mm ≥6 Adjacent pixels (≥2 mm 2 ) South Bay Heart Watch Park et al. 2002 1461 EBCT (Imatron C-100) 80% R-R interval — — — 6.0 mm See MESA (≥4.1 mm 3 ) Qu et al. 2003 1312 EBCT (Imatron C-100) 80% R-R interval 100 ms Exposure — — 6.0 mm
3.0 mm ( n = 319 Validation purposes) See MESA Greenland et al. 2004 1461 (EB) CT — — — — 6.0 mm See MESA — Shaw et al.
Raggi et al. 2003
2004 10,377 EBCT (Imatron C-100, Imatron C-150) 60%–80% R-R interval 100 ms — — 3.0 mm Slice thickness
contiguous Threshold: 130 HU ≥3 contiguous pixels (1.03 mm 3 ) — Kondos et al. 2003 8855 EBCT (Imatron C-100) 80% R-R interval 100 ms — — 3.0 mm, FOV 260 mm, 512 matrix, sharp kernel Threshold: 130 HU ≥4 adjacent pixels (1.0 mm 2 ) Cooper Clinic Dallas Cheng et al. 2003 17,967 EBCT (Siemens Evolution C-150XP) — 100 ms — — 3.0 mm Slice thickness
2.0 mm Increment — LaMonte et al. 2005 10,746 EBCT — — — — — — Church et al. 2007 10,746 EBCT (Imatron C-150 XP, Imatron C-300) — — — — 3.0 mm Slice thickness
2.0 mm Increment — MESA Carr et al. 2005 6814 EBCT
MDCT Prospective, 80% R-R
Prospective, 50% R-R
Prospective, 50% R-R
Retrospective, 50% R-R Sequential mode
MDCT: 4 detect row
Sequential
Sequential
Sequential 130 kVp
140 kVp
120 kVp
120 kVp 63 mAs
50 mAs
106 mAs
320 mAs 3.0 mm, FOV 350 mm
2.5 mm, FOV 350 mm ≥5.5 mm 3
≥4.6 mm 3 Rotterdam Coronary Calcification Study Vliegenthart et al. 2005 1795 EBCT (Imatron C-150) 80% R-R interval 100 ms/slice — — 3.0 mm Threshold: 130 HU
≥2 adjacent pixels (0.65 mm 2 ) PACC project Taylor et al. 2005 2000 EBCT (Imatron C-150 LXP) 60%–80% R-R interval — — — 3.0 mm Slice thickness Threshold: 130 HU
≥4 contiguous pixels Framingham Heart Study Moselewski et al. 2005 612 8-Slice MDCT(Lightspeed Ultra GE) 50% R-R interval Sequential 120 kVp 320 mA
400 mA 2.5 mm Slice thickness
contiguous Threshold: 130 HU
≥3 connected pixels HNR, ECAC Schmermund et al. 2007 Ongoing EBCT (Imatron C-100, Imatron C-150) 80% R-R interval 100 ms 3.0 mm Slice thickness
Contiguous Threshold: 130 HU
≥4 contiguous pixels CONFIRM registry Min et al. 2011 27,125 MDCT, DSCT — — — — — — SCOT-HEART Newby et al. 2012 ~2070 64, 128, 320 MDCT — — — — — Threshold: 130 HU Jackson Heart Study Liu et al. 2012 2880 MDCT (Lightspeed 16 Pro, GE) — — — — — — NHLBI Family Heart study Robbins et al. 2014 1848 MDCT 50% R-R interval Sequential, 0.5 s gantry rotation, temporal res. 250–300 ms 120 kV 160 mAs 2.5 mm, FOV 350 mm Threshold: 130 HU
≥2 connected pixels (0.9 mm) ROMICAT II trial Pursnani et al. 2015 473 MDCT, DSCT
GE 64-Slice Lightspeed, GE Lightspeed VCT, Siemens 64-Slice Sensation, Siemens Dual Source 64-Slice Definition, Siemens Dual Source 128-Slice Flash, and Philips Brilliance 256-Slice iCT — — — — — — EURO-CCAD Nicoll et al. 2016 5515 MDCT — 4–256 slices — — 3.0 mm ≥4 Contiguous pixels CRESCENT Lubbers et al. 2016 242 CT — — — — — —
CARDIA, Coronary Artery Risk Development in Young Adults; CONFIRM, COroNary CT Angiography Evaluation For Clinical Outcomes: An InteRnational Multicenter Registry; CRESCENT, Computed Tomography vs. Exercise Testing in Suspected Coronary Artery Disease; CT, computed tomography; DSCT, dual-source computed tomography; EBCT, electron beam computed tomography; ECAC, Epidemiology of Coronary Calcification; ECG, electrocardiography; EURO-CCAD, European Calcific Coronary Artery Disease; FOV, field of view; MDCT, multidetector computed tomography; MESA, Multi-Ethnic Study of Atherosclerosis; PACC, Prospective Army Coronary Calcium; ROMICAT, Rule Out Myocardial Infarction using Computer Assisted Tomography; SCOT-HEART, Scottish COmputed Tomography of the HEART trial.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Impact of Parameter Settings on CAC Score
Get Radiology Tree app to read full this article<
Screenee Characteristics
Get Radiology Tree app to read full this article<
Heart Rate and Vessel Displacement
Get Radiology Tree app to read full this article<
Electrocardiography (ECG) Triggering
Get Radiology Tree app to read full this article<
Tube Voltage
Get Radiology Tree app to read full this article<
Tube Current
Get Radiology Tree app to read full this article<
Slice Thickness and Increment
Get Radiology Tree app to read full this article<
Kernel/FOV
Get Radiology Tree app to read full this article<
Iterative Reconstruction
Get Radiology Tree app to read full this article<
Scoring Software
Get Radiology Tree app to read full this article<
Design CAC Imaging Protocol
Preparation
Get Radiology Tree app to read full this article<
Acquisition
Get Radiology Tree app to read full this article<
TABLE 2
CT Acquisition Protocol for CAC Scoring Scan
Scan Parameters CT Protocol A B Scan mode High pitch spiral Sequential Pitch 3.4 — Tube voltage (kVp) 120 Tube current (ref. mAs) 80 Rotation time (ms) 280 Collimation (mm) 128 × 0.6 Matrix 512 × 512 ECG triggering Prospective, 60% Dose modulation CareDose 4D → semi →enter ref mAs API Inspiratory breath-hold Direction Craniocaudal Upper limit Below carina Lower limit Apex/bottom edge heart
API, automated patient instruction; CAC, coronary artery calcium; CT, computed tomography; ECG, electrocardiography.
Get Radiology Tree app to read full this article<
Reconstruction
Get Radiology Tree app to read full this article<
TABLE 3
CT Reconstruction Protocol for CAC Scoring Scan
Reconstruction Parameters Protocols A and B Reconstruction 1 Reconstruction 2 Reconstruction 3 Slice thickness (mm) 3.0 1.5 3.0 Slice increment (mm) 1.5 1.0 1.5 FOV (mm) 250 250 Maximum Kernel b35f (sharp) Algorithm Filtered-back projection Window Mediastinum Window width (HU) 350 Window center (HU) 50
CAC, coronary artery calcium; CT, computed tomography; ECG, electrocardiography; FOV, field of view.
Get Radiology Tree app to read full this article<
Analysis
Get Radiology Tree app to read full this article<
Design Imaging Data Management
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
TABLE 4
Incidental Findings on CT Scan for CAC Scoring That Are (Not) Reported to GP and Participant
Reported Not Reported Chest
Abdomen
CAC, coronary artery calcium; CT, computed tomography; GP, general practitioner.
TABLE 5
Cardiovascular Risk Stratification Based on the CAC Score
Calcium Score Extent of Atherosclerotic Coronary Artery Disease Cardiovascular Disease Risk 0 No identifiable plaque Low 1–10 Mild identifiable plaque Low 11–99 Definite, at least mild atherosclerotic plaque Low 100–399 Definite, at least moderate atherosclerotic plaque High ≥400 Extensive atherosclerotic plaque Very high
CAC, coronary artery calcium.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Greenland P., Alpert J.S., Beller G.A., et. al.: 2010 ACCF/AHA guideline for assessment of cardiovascular risk in asymptomatic adults: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation 2010; 122: pp. 2748-2764.
2. Perk J., De Backer G., Gohlke H., et. al.: European Guidelines on cardiovascular disease prevention in clinical practice (version 2012). Eur Heart J 2012; 33: pp. 1635-1701.
3. Silverman M.G., Blaha M.J., Krumholz H.M., et. al.: Impact of coronary artery calcium on coronary heart disease events in individuals at the extremes of traditional risk factor burden: the Multi-Ethnic Study of Atherosclerosis. Eur Heart J 2014; 35: pp. 2232-2241.
4. Elias-Smale S.E., Proena R.V., Koller M.T., et. al.: Coronary calcium score improves classification of coronary heart disease risk in the elderly: the Rotterdam study. J Am Coll Cardiol 2010; 56: pp. 1407-1414.
5. Oudkerk M., Stillman A.E., Halliburton S.S., et. al.: Coronary artery calcium screening: current status and recommendations from the European Society of Cardiac Radiology and North American Society for Cardiovascular Imaging. Int J Cardiovasc Imaging 2008; 24: pp. 645-671.
6. Piepoli M.F., Hoes A.W., Agewall S., et. al.: 2016 European Guidelines on cardiovascular disease prevention in clinical practice. Eur Heart J 2016; 37: pp. 2315-2381.
7. McEvoy J.W., Martin S.S., Blaha M.J., et. al.: The case for and against a coronary artery calcium trial. J Am Coll Cardiol Img 2016; 9: pp. 994-1002.
8. Kim K.P., Einstein A.J., Berrington de Gonzalez A.: Coronary artery calcification screening: estimated radiation dose and cancer risk. Arch Intern Med 2009; 169: pp. 1188-1194.
9. Baron K.B., Choi A.D., Chen M.Y.: Low radiation dose calcium scoring: evidence and techniques. Curr Cardiovasc Imaging Rep 2016;
10. Sullivan D.C., Obuchowski N.A., Kessler L.G., et. al.: Metrology standards for quantitative imaging biomarkers. Radiology 2015; 277: pp. 813-825.
11. Agatston A.S., Janowitz F.W.R., Hildner F.J., et. al.: Quantification of coronary artery calcium using ultrafast computed tomography. JACC 1990; 15: pp. 827-832.
12. Arad Y., Spadaro L.A., Goodman K., et. al.: Prediction of coronary events with electron beam computed tomography. J Am Coll Cardiol 2000; 36: pp. 1253-1260.
13. Arad Y., Newstein D., Roth M., et. al.: Rationale and design of the St. Francis Heart Study: a randomized clinical trial of atorvastatin plus antioxidants in asymptomatic persons with elevated coronary calcification. Control Clin Trials 2001; 22: pp. 553-572.
14. Iribarren C., Sidney S., Bild D.E., et. al.: Association of hostility with coronary artery calcification in young adults. JAMA 2000; 283: pp. 2546.
15. Carr J.J., Nelson J.C., Wong N.D., et. al.: Calcified coronary artery plaque measurement with cardiac CT in population-based studies: standardized protocol of Multi-Ethnic Study of Atherosclerosis (MESA) and Coronary Artery Risk Development in Young Adults (CARDIA) Study 1. Radiology 2005; 234: pp. 35-43.
16. Yan L.L., Liu K., Daviglus M.L., et. al.: Education, 15-year risk factor progression, and coronary artery calcium in young adulthood and early middle age. JAMA 2006; 295: pp. 1793.
17. Park R.: Combined use of computed tomography coronary calcium scores and C-Reactive protein levels in predicting cardiovascular events in nondiabetic individuals. Circulation 2002; 106: pp. 2073-2077.
18. Qu W., Le T.T., Azen S.P., et. al.: Value of coronary artery calcium scanning by computed tomography for predicting coronary heart disease in diabetic subjects. Diabetes Care 2003; 26: pp. 905-910.
19. Greenland P.: Coronary artery calcium score combined with Framingham score for risk prediction in asymptomatic individuals. JAMA 2004; 291: pp. 210.
20. Shaw L.J., Raggi P., Schisterman E., et. al.: Prognostic value of cardiac risk factors and coronary artery calcium screening for all-cause mortality. Radiology 2003; 228: pp. 826-833.
21. Raggi P., Shaw L.J., Berman D.S., et. al.: Prognostic value of coronary artery calcium screening in subjects with and without diabetes. J Am Coll Cardiol 2004; 43: pp. 1663-1669.
22. Kondos G.T.: Electron-beam tomography coronary artery calcium and cardiac events: a 37-month follow-up of 5635 initially asymptomatic low- to intermediate-risk adults. Circulation 2003; 107: pp. 2571-2576.
23. Cheng Y.J., Church T.S., Kimball T.E., et. al.: Comparison of coronary artery calcium detected by electron beam tomography in patients with to those without symptomatic coronary heart disease. Am J Cardiol 2003; 92: pp. 498-503.
24. LaMonte M.J.: Coronary artery calcium score and coronary heart disease events in a large cohort of asymptomatic men and women. Am J Epidemiol 2005; 162: pp. 421-429.
25. Church T.S., Levine B.D., McGuire D.K., et. al.: Coronary artery calcium score, risk factors, and incident coronary heart disease events. Atherosclerosis 2007; 190: pp. 224-231. S0021-9150(06)00058-X [pii]
26. Vliegenthart R.: Coronary calcification improves cardiovascular risk prediction in the elderly. Circulation 2005; 112: pp. 572-577.
27. Taylor A.J., Bindeman J., Feuerstein I., et. al.: Coronary calcium independently predicts incident premature coronary heart disease over measured cardiovascular risk factors. J Am Coll Cardiol 2005; 46: pp. 807-814.
28. Moselewski F.: Calcium concentration of individual coronary calcified plaques as measured by multidetector row computed tomography. Circulation 2005; 111: pp. 3236-3241.
29. Schmermund A., Lehmann N., Bielak L.F., et. al.: Comparison of subclinical coronary atherosclerosis and risk factors in unselected populations in Germany and US-America. Atherosclerosis 2007; 195: pp. e207-e216.
30. Min J.K., Dunning A., Lin F.Y., et. al.: Rationale and design of the CONFIRM (COroNary CT Angiography EvaluatioN For Clinical Outcomes: an InteRnational Multicenter) registry. J Cardiovasc Comput Tomogr 2011; 5: pp. 84-92.
31. Newby D.E., Williams M.C., Flapan A.D., et. al.: Role of multidetector computed tomography in the diagnosis and management of patients attending the rapid access chest pain clinic, The Scottish COmputed Tomography of the HEART (SCOT-HEART) trial: study protocol for randomized controlled trial. Trials 2012; 13: pp. 184.
32. Liu J., Musani S.K., Bidulescu A., et. al.: Fatty liver, abdominal adipose tissue and atherosclerotic calcification in African Americans: the Jackson Heart Study. Atherosclerosis 2012; 224: pp. 521-525.
33. Robbins J.M., Petrone A.B., Ellison R.C., et. al.: Association of egg consumption and calcified atherosclerotic plaque in the coronary arteries: the NHLBI Family Heart Study. ESPEN J 2014; 9: pp. e131-e135.
34. Pursnani A., Chou E.T., Zakroysky P., et. al.: Use of coronary artery calcium scanning beyond coronary computed tomographic angiography in the emergency department evaluation for acute chest pain: the ROMICAT II Trial. Circ Cardiovasc Imaging 2015; 8: pp. e002225.
35. Nicoll R., Wiklund U., Zhao Y., et. al.: Gender and age effects on risk factor-based prediction of coronary artery calcium in symptomatic patients: a Euro-CCAD study. Atherosclerosis 2016; 252: pp. 32-39.
36. Lubbers M., Dedic A., Coenen A., et. al.: Calcium imaging and selective computed tomography angiography in comparison to functional testing for suspected coronary artery disease: the multicentre, randomized CRESCENT trial. Eur Heart J 2016; 37: pp. 1232-1243.
37. Newton T.D., Mehrez H., Wong K., et. al.: Radiation dose threshold for coronary artery calcium score with MDCT: how low can you go?. Eur Radiol 2011; 21: pp. 2121-2129.
38. Nelson J.C., Kronmal R.A., Carr J.J., et. al.: Measuring coronary calcium on CT images adjusted for attenuation differences. Radiology 2005; 235: pp. 403-414.
39. Stanford W., Burns T.L., Thompson B.H., et. al.: Influence of body size and section level on calcium phantom measurements at coronary artery calcium CT scanning. Radiology 2004; 230: pp. 198-205.
40. Qian Z., Joshi P.H., Shaukat A.F., et. al.: Relationship between chest lateral width, tube current, image noise, and radiation exposure associated with coronary artery calcium scanning on 320-detector row CT. J Cardiovasc Comput Tomogr 2011; 5: pp. 231-239.
41. Willemink M.J., Abramiuc B., den Harder A.M., et. al.: Coronary calcium scores are systematically underestimated at a large chest size: a multivendor phantom study. J Cardiovasc Comput Tomogr 2015; 9: pp. 1-7.
42. Li Q., Liu S., Myers K.J., et. al.: Impact of reconstruction algorithms and gender-associated anatomy on coronary calcium scoring with CT. Acad Radiol 2016; 23: pp. 1470-1479.
43. Tigges S., Arepalli C.D., Tridandapani S., et. al.: A phantom study of the effect of heart rate, coronary artery displacement and vessel trajectory on coronary artery calcium score: potential for risk misclassification. J Cardiovasc Comput Tomogr 2012; 6: pp. 260-267.
44. Groen J.M., Greuter M.J., Schmidt B., et. al.: The influence of heart rate, slice thickness, and calcification density on calcium scores using 64-slice multidetector computed tomography: a systematic phantom study. Invest Radiol 2007; 42: pp. 848-855.
45. Ulzheimer S., Kalender W.A.: Assessment of calcium scoring performance in cardiac computed tomography. Eur Radiol 2003; 13: pp. 484-497.
46. Funabashi N., Irie R., Namihira Y., et. al.: Influence of tube voltage and heart rate on the Agatston calcium score using an in vitro, novel ECG-gated dual energy reconstruction 320 slice CT technique. Int J Cardiol 2015; 180: pp. 218-220.
47. Rutten A., Krul S.P.J., Meijs M.F.L., et. al.: Variability of coronary calcium scores throughout the cardiac cycle: implications for the appropriate use of electrocardiogram-dose modulation with retrospectively gated computed tomography. Invest Radiol 2008; 43: pp. 187-194.
48. Matsuura N., Horiguchi J., Yamamoto H., et. al.: Optimal cardiac phase for coronary artery calcium scoring on single-source 64-MDCT scanner: least interscan variability and least motion artifacts. Am J Roentgenol 2008; 190: pp. 1561-1568.
49. Deprez F.C., Vlassenbroek A., Raaijmakers R., et. al.: Controversies about effects of low-kilovoltage MDCT acquisition on Agatston calcium scoring. J Cardiovasc Comput Tomogr 2013; 7: pp. 58-61.
50. Blobel J., Mews J., Goatman K.A., et. al.: Calibration of coronary calcium scores determined using iterative image reconstruction (AIDR 3D) at 120, 100, and 80 kVp. Med Phys 2016; 43: pp. 1921-1932.
51. Fujioka C., Funama Y., Kiguchi M., et. al.: Coronary artery calcium scoring on different 64-detector scanners using a low-tub voltage (80 kVp). Acad Radiol 2012; 19: pp. 1402-1407.
52. Nakazato R., Dey D., Gutstein A., et. al.: Coronary artery calcium scoring using a reduced tube voltage and radiation dose protocol with dual-source computed tomography. J Cardiovasc Comput Tomogr 2009; 3: pp. 394-400.
53. Marwan M., Seltmann M., Pflederer T., et. al.: Very low-dose coronary artery calcium score using high-pitch spiral acquisition mode: comparison between standard 120 kV versus 100 kV tube voltage protocols. J Cardiovasc Comput Tomogr 2010; 4: pp. S61.
54. Thomas C.K., Mühlenbruch G., Wildberger J.E., et. al.: Coronary artery calcium scoring with multislice computed tomography: in vitro assessment of a low tube voltage protocol. Invest Radiol 2006; 41: pp. 668-673.
55. Dey D., Nakazato R., Pimentel R., et. al.: Low radiation coronary calcium scoring by dual-source CT with tube current optimization based on patient body size. J Cardiovasc Comput Tomogr 2012; 6: pp. 113-120.
56. Hong C., Bae K., Pilgram T.K., et. al.: Coronary artery calcium measurement with multi–detector row CT: in vitro assessment of effect of radiation dose. Radiology 2002; 225: pp. 901-906.
57. Horiguchi J., Matsuura N., Yamamoto H., et. al.: Evaluation of attenuation-based tube current control in coronary artery calcium scoring on prospective ECG-triggered 64-detector CT. Acad Radiol 2009; 16: pp. 1231-1240.
58. Mühlenbruch G., Hohl C., Das M., et. al.: Evaluation of automated attenuation-based tube current adaptation for coronary calcium scoring in MDCT in a cohort of 262 patients. Eur Radiol 2007; 17: pp. 1850-1857.
59. Qian Z., Dhungel A., Vazquez G., et. al.: Coronary artery calcium: 0.5 mm slice-thickness reconstruction with adjusted attenuation threshold outperforms 3.0 mm by validating against spatially registered intravascular ultrasound with radiofrequency backscatter. Acad Radiol 2015; 22: pp. 1128-1137.
60. Aslam A., Khokhar U.S., Chaudhry A., et. al.: Assessment of isotropic calcium using 0.5-mm reconstructions from 320-row CT data sets identifies more patients with non-zero Agatston score and more subclinical atherosclerosis than standard 3.0-mm coronary artery calcium scan and CT angiography. J Cardiovasc Comput Tomogr 2014; 8: pp. 58-66.
61. Mühlenbruch G., Thomas C., Wildberger J.E., et. al.: Effect of varying slice thickness on coronary calcium scoring with multislice computed tomography in vitro and in vivo. Invest Radiol 2005; 40: pp. 695-699.
62. van der Bijl N., de Bruin P.W., Geleijns J., et. al.: Assessment of coronary artery calcium by using volumetric 320-row multi-detector computed tomography: comparison of 0.5 mm with 3.0 mm slice reconstructions. Int J Cardiovasc Imaging 2010; 26: pp. 473-482.
63. Rutten A., Isgum I., Prokop M.: Calcium scoring with prospectively ECG-triggered CT: using overlapping datasets generated with MPR decreases inter-scan variability. Eur J Radiol 2011; 80: pp. 83-88.
64. Horiguchi J., Matsuura N., Yamamoto H., et. al.: Variability of repeated coronary artery calcium measurements by 1.25-mm- and 2.5-mm-thickness images on prospective electrocardiograph-triggered 64-slice CT. Eur Radiol 2008; 18: pp. 209-216.
65. Vliegenthart R., Hofman A., Witteman J.C.M.: Radiology coronary calcification at electron-beam CT: effect of section thickness on calcium scoring in vitro and in vivo 1. Radiology 2003; 229: pp. 520-525.
66. Schlosser T., Hunold P., Voigtländer T., et. al.: Coronary artery calcium scoring: influence of reconstruction interval and reconstruction increment using 64-MDCT. Am J Roentgenol 2007; 188: pp. 1063-1068.
67. Mahnken A.H., Wildberger J.E., Sinha A.M., et. al.: Variation of the coronary calcium score depending on image reconstruction interval and scoring algorithm. Invest Radiol 2002; 37: pp. 496-502.
68. Achenbach S., Meissner F., Ropers D., et. al.: Overlapping cross-sections significantly improve the reproducibility of coronary calcium measurements by electron beam tomography: a phantom study. J Comput Assist Tomogr 2001; 25: pp. 569-573. 00004728-200107000-00010
69. Groen J.M., Kofoed K.F., Zacho M., et. al.: Calcium score of small coronary calcifications on multidetector computed tomography: results from a static phantom study. Eur J Radiol 2013; 82: pp. e58-e63.
70. Mahnken A.H., Mühlenbruch G., Koos R., et. al.: Influence of a small field-of-view size on the detection of coronary artery calcifications with MSCT: in vitro and in vivo study. Eur Radiol 2006; 16: pp. 358-364.
71. Choi A.D., Leifer E.S., Yu J., et. al.: Prospective evaluation of the influence of iterative reconstruction on the reproducibility of coronary calcium quantification in reduced radiation dose 320 detector row CT. J Cardiovasc Comput Tomogr 2016; 10: pp. 359-363.
72. McQuiston A.D., Muscogiuri G., Schoepf U.J., et. al.: Approaches to ultra-low radiation dose coronary artery calcium scoring based on 3rd generation dual-source CT: a phantom study. Eur J Radiol 2016; 85: pp. 39-47.
73. van Osch J.A.C., Mouden M., van Dalen J.A., et. al.: Influence of iterative image reconstruction on CT-based calcium score measurements. Int J Cardiovasc Imaging 2014; 30: pp. 961-967.
74. Blobel J., Mews J., Schuijf J.D., et. al.: Determining the radiation dose reduction potential for coronary calcium scanning with computed tomography the adaptive iterative dose reduction algorithm for image reconstruction. Invest Radiol 2013; 48: pp. 857-862.
75. Willemink M.J., den Harder A.M., Foppen W., et. al.: Finding the optimal dose reduction and iterative reconstruction level for coronary calcium scoring. J Cardiovasc Comput Tomogr 2015; 10: pp. 69-75.
76. Takahashi M., Kimura F., Umezawa T., et. al.: Comparison of adaptive statistical iterative and filtered back projection reconstruction techniques in quantifying coronary calcium. J Cardiovasc Comput Tomogr 2015; 1–8:
77. Matsuura N., Urashima M., Fukumoto W., et. al.: Radiation dose reduction at coronary artery calcium scoring by using a low tube current technique and hybrid iterative reconstruction. J Comput Assist Tomogr 2015; 39: pp. 119-124.
78. Tatsugami F., Higaki T., Fukumoto W., et. al.: Radiation dose reduction for coronary artery calcium scoring at 320-detector CT with adaptive iterative dose reduction 3D. Int J Cardiovasc Imaging 2015; 31: pp. 1045-1052.
79. Obmann V.C., Klink T., Heverhagen J.T., et. al.: Impact of hybrid iterative reconstruction on Agatston coronary artery calcium scores in comparison to filtered back projection in native cardiac CT. Fortschr Röntgenstr 2015; 187: pp. 372-379.
80. Schindler A., Vliegenthart R., Schoepf U.J., et. al.: Iterative image reconstruction techniques for CT coronary artery calcium quantification: comparison with traditional filtered back projection in vitro and in vivo. Radiology 2014; 270: pp. 387-393.
81. Willemink M.J., Takx R.A.P., de Jong P.A., et. al.: The impact of CT radiation dose reduction and iterative reconstruction algorithms from four different vendors on coronary calcium scoring. Eur Radiol 2014; 24: pp. 2201-2212.
82. Den Harder A.M., Willemink M.J., Bleys R.L.A.W., et. al.: Dose reduction for coronary calcium scoring with hybrid and model-based iterative reconstruction: an ex vivo study. Int J Cardiovasc Imaging 2014; 30: pp. 1125-1133.
83. Gebhard C., Fiechter M., Fuchs T.A., et. al.: Coronary artery calcium scoring: Influence of adaptive statistical iterative reconstruction using 64-MDCT. Int J Cardiol 2013; 167: pp. 2932-2937.
84. Weininger M., Ritz K.S., Schoepf U.J., et. al.: Interplatform reproducibility of CT coronary calcium scoring software. Radiology 2012; 265: pp. 70-77.
85. van Ooijen P.M.A., Vliegenthart R., Witteman J.C., et. al.: Influence of scoring parameter settings on Agatston and volume scores for coronary calcification. Eur Radiol 2005; 15: pp. 102-110.
86. McCollough C.H., Ulzheimer S., Halliburton S.S., et. al.: Coronary artery calcium: a multi-institutional, multimanufacturer international standard for quantification at cardiac CT. Radiology 2007; 243: pp. 527-538.