
Rationale and Objectives
This study aims to compare the image quality of coronary artery stent scans on computed tomography images reconstructed with forward projected model-based iterative reconstruction solution (FIRST) and adaptive iterative dose reduction 3D (AIDR 3D).
Materials and Methods
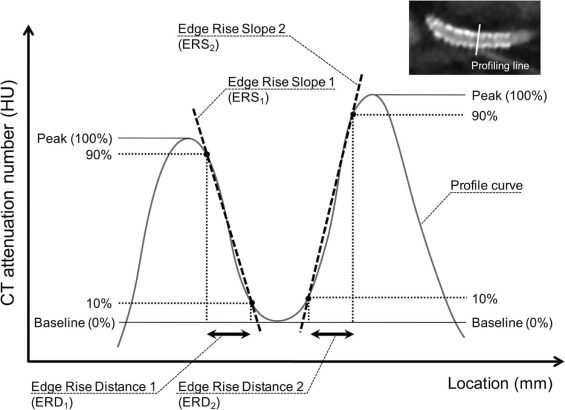
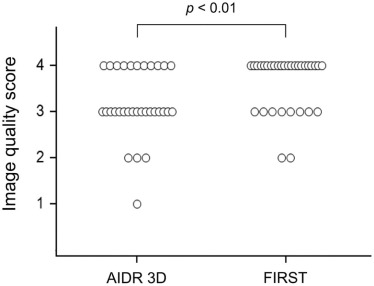
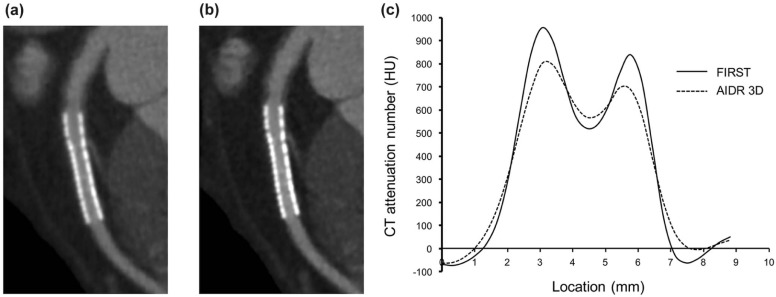
Coronary computed tomography angiography scans of 23 patients with 32 coronary stents were used. The images were reconstructed with AIDR 3D and FIRST. We generated computed tomography attenuation profiles across the stents and measured the width of the edge rise distance and the edge rise slope (ERS). We also calculated the stent lumen attenuation increase ratio (SAIR) and measured visible stent lumen diameters. Two radiologists visually evaluated the image quality of the stents using a 4-point scale (1 = poor, 4 = excellent).
Results
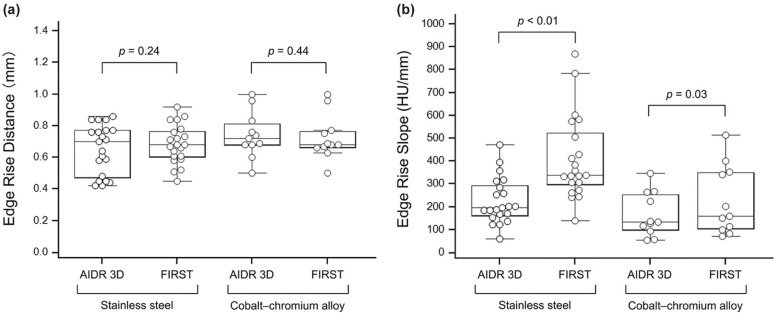
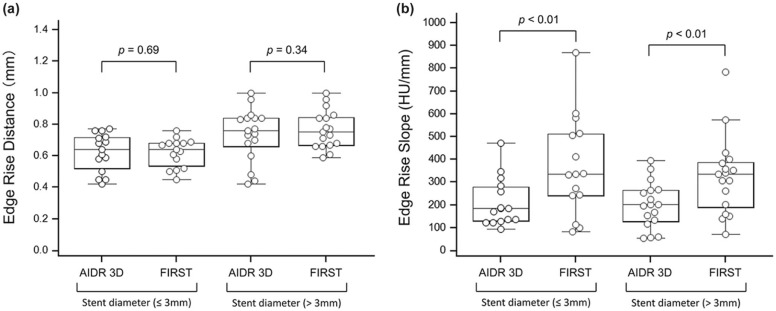
There was no significant difference in the edge rise distance between the two reconstruction methods ( P = 0.36). The ERS on FIRST images was greater than the ERS on AIDR 3D images (325.2 HU/mm vs 224.4 HU/mm; P < 0.01). The rate of the visible stent lumen diameter compared to the true diameter on FIRST images was higher than that on AIDR 3D images (51.4% vs 47.3%, P < 0.01). The SAIR on FIRST images was lower than the SAIR on AIDR 3D images (0.19 vs 0.30, P < 0.01). The mean image quality scores for AIDR 3D and FIRST images were 3.18 and 3.63, respectively; the difference was also significant ( P < 0.01).
Conclusion
The image quality of coronary artery stent scans is better on FIRST than on AIDR 3D images.
Introduction
Coronary computed tomography angiography (CTA) is a suitable noninvasive imaging modality for patient follow-up after coronary artery stent implantation . However, blooming artifacts from stent struts limit the evaluation of stent lumens . These artifacts primarily arise from partial volume averaging and beam hardening; stent struts appear thicker than they are and often overlap the vessel lumen , which complicates assessment of coronary artery stent patency.
Advances in computer processing hardware have made it possible to use the iterative reconstruction (IR) algorithm in the clinical setting for computed tomography (CT) studies. Hybrid IR, which applies noise reduction techniques to the raw data and image domains, has been shown to be superior to conventional filtered back projection (FBP) because it reduces blooming artifacts and improves the image quality of coronary artery stent scans . Model-based IR has been introduced as a new reconstruction algorithm. The advantage of model-based IR is higher spatial resolution compared to images reconstructed with conventional FBP or hybrid IR , and its sophisticated modeling is expected to reduce blooming artifacts and improve the image quality compared to hybrid IR.
Get Radiology Tree app to read full this article<
Materials and Methods
Patients
Get Radiology Tree app to read full this article<
CT Scanning
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Quantitative Analysis
Get Radiology Tree app to read full this article<
Sharpness of the Stent Struts
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Attenuation Effects of the Stent Struts
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Image Noise
Get Radiology Tree app to read full this article<
Qualitative Analysis
Get Radiology Tree app to read full this article<
Statistical Analyses
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
TABLE 1
Stent Characteristics
Name Manufacturer Material Nominal Stent Diameter (mm) 2.5 2.75 3.0 3.5 4.0 Xience Abbott Vascular Stainless steel 1 2 2 3 3 Cypher Cordis Stainless steel 1 0 3 1 0 Integrity Medtronic Cobalt-chromium alloy 0 1 2 1 1 Nobori Terumo Stainless steel 1 0 1 2 0 Driver Medtronic Cobalt-chromium alloy 0 1 0 2 1 Multi-Link 8 Abbott Cobalt-chromium alloy 0 0 0 2 0 Taxus Boston Scientific Stainless steel 0 0 0 1 0 Total 3 4 8 12 5
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
TABLE 2
Overall Quantitative Image Quality Parameters
AIDR 3D FIRST_P_ ERD mean (mm) 0.67 (0.30–1.64) 0.69 (0.45–1.64) 0.36 ERS mean (HU/mm) 224.4 (46.4–477.1) 325.2 (61.9–876.4) <0.01 SAIR 0.30 (0.04–1.08) 0.19 (0.01–0.55) <0.01 Visible diameter (%) 47.3 (31.4–76.4) 51.4 (36.0–80.0) <0.01 Image noise (HU) 24.6 (19.2–31.9) 23.4 (19.9–28.3) 0.17
AIDR 3D, adaptive iterative dose reduction 3D; ERD, edge rise distance; ERS, edge rise slope; FIRST, forward projected model-based iterative reconstruction solution; SAIR, stent lumen attenuation increase ratio.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Taylor A.J., Cerqueira M., Hodgson J.M., et. al.: ACCF/SCCT/ACR/AHA/ASE/ASNC/NASCI/SCAI/SCMR 2010 appropriate use criteria for cardiac computed tomography. A report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, the Society of Cardiovascular Computed Tomography, the American College of Radiology, the American Heart Association, the American Society of Echocardiography, the American Society of Nuclear Cardiology, the North American Society for Cardiovascular Imaging, the Society for Cardiovascular Angiography and Interventions, and the Society for Cardiovascular Magnetic Resonance. J Am Coll Cardiol 2010; 56: pp. 1864-1894.
2. Schuijf J.D., Pundziute G., Jukema J.W., et. al.: Evaluation of patients with previous coronary stent implantation with 64-section CT. Radiology 2007; 245: pp. 416-423.
3. Cademartiri F., Schuijf J.D., Pugliese F., et. al.: Usefulness of 64-slice multislice computed tomography coronary angiography to assess in-stent restenosis. J Am Coll Cardiol 2007; 49: pp. 2204-2210.
4. Manghat N., Van Lingen R., Hewson P., et. al.: Usefulness of 64-detector row computed tomography for evaluation of intracoronary stents in symptomatic patients with suspected in-stent restenosis. Am J Cardiol 2008; 101: pp. 1567-1573.
5. de Graaf F.R., Schuijf J.D., van Velzen J.E., et. al.: Diagnostic accuracy of 320-row multidetector computed tomography coronary angiography to noninvasively assess in-stent restenosis. Invest Radiol 2010; 45: pp. 331-340.
6. Pugliese F., Cademartiri F., van Mieghem C., et. al.: Multidetector CT for visualization of coronary stents. Radiographics 2006; 26: pp. 887-904.
7. Ebersberger U., Tricarico F., Schoepf U.J., et. al.: CT evaluation of coronary artery stents with iterative image reconstruction: improvements in image quality and potential for radiation dose reduction. Eur Radiol 2013; 23: pp. 125-132.
8. Gebhard C., Fiechter M., Fuchs T.A., et. al.: Coronary artery stents: influence of adaptive statistical iterative reconstruction on image quality using 64-HDCT. Eur Heart J Cardiovasc Imaging 2013; 14: pp. 969-977.
9. Nelson R.C., Feuerlein S., Boll D.T.: New iterative reconstruction techniques for cardiovascular computed tomography: how do they work, and what are the advantages and disadvantages?. J Cardiovasc Comput Tomogr 2011; 5: pp. 286-292.
10. Geyer L.L., Schoepf U.J., Meinel F.G., et. al.: State of the art: iterative CT reconstruction techniques. Radiology 2015; 276: pp. 339-357.
11. Thibault J.B., Sauer K.D., Bouman C.A., et. al.: A three-dimensional statistical approach to improved image quality for multislice helical CT. Med Phys 2007; 34: pp. 4526-4544.
12. Hausleiter J., Meyer T., Hermann F., et. al.: Estimated radiation dose associated with cardiac CT angiography. JAMA 2009; 301: pp. 500-507.
13. Yang W.J., Pan Z.L., Zhang H., et. al.: Evaluation of coronary artery in-stent restenosis with prospectively ECG-triggered axial CT angiography versus retrospective technique: a phantom study. Radiol Med (Torino) 2011; 116: pp. 189-196.
14. Kumbhani D.J., Ingelmo C.P., Schoenhagen P., et. al.: Meta-analysis of diagnostic efficacy of 64-slice computed tomography in the evaluation of coronary in-stent restenosis. Am J Cardiol 2009; 103: pp. 1675-1681.
15. Gervaise A., Osemont B., Lecocq S., et. al.: CT image quality improvement using adaptive iterative dose reduction with wide-volume acquisition on 320-detector CT. Eur Radiol 2012; 22: pp. 295-301.
16. Tomizawa N., Nojo T., Akahane M., et. al.: Adaptive iterative dose reduction in coronary CT angiography using 320-row CT: assessment of radiation dose reduction and image quality. J Cardiovasc Comput Tomogr 2012; 6: pp. 318-324.
17. Hou Y., Xu S., Guo W., et. al.: The optimal dose reduction level using iterative reconstruction with prospective ECG-triggered coronary CTA using 256-slice MDCT. Eur J Radiol 2012; 81: pp. 3905-3911.
18. Takx R.A., Schoepf U.J., Moscariello A., et. al.: Coronary CT angiography: comparison of a novel iterative reconstruction with filtered back projection for reconstruction of low-dose CT-Initial experience. Eur J Radiol 2013; 82: pp. 275-280.
19. Fuchs T.A., Fiechter M., Gebhard C., et. al.: CT coronary angiography: impact of adapted statistical iterative reconstruction (ASIR) on coronary stenosis and plaque composition analysis. Int J Cardiovasc Imaging 2013; 29: pp. 719-724.
20. Maintz D., Seifarth H., Raupach R., et. al.: 64-slice multidetector coronary CT angiography: in vitro evaluation of 68 different stents. Eur Radiol 2006; 16: pp. 818-826.
21. Maintz D., Burg M.C., Seifarth H., et. al.: Update on multidetector coronary CT angiography of coronary stents: in vitro evaluation of 29 different stent types with dual-source CT. Eur Radiol 2009; 19: pp. 42-49.
22. Gassenmaier T., Petri N., Allmendinger T., et. al.: Next generation coronary CT angiography: in vitro evaluation of 27 coronary stents. Eur Radiol 2014; 24: pp. 2953-2961.
23. Mieville F.A., Gudinchet F., Brunelle F., et. al.: Iterative reconstruction methods in two different MDCT scanners: physical metrics and 4-alternative forced-choice detectability experiments—a phantom approach. Phys Med 2013; 29: pp. 99-110.
24. Millon D., Vlassenbroek A., Van Maanen A.G., et. al.: Low contrast detectability and spatial resolution with model-based Iterative reconstructions of MDCT images: a phantom and cadaveric study. Eur Radiol 2016;
25. Oda S., Weissman G., Vembar M., et. al.: Iterative model reconstruction: improved image quality of low-tube-voltage prospective ECG-gated coronary CT angiography images at 256-slice CT. Eur J Radiol 2014; 83: pp. 1408-1415.
26. Iyama Y., Nakaura T., Kidoh M., et. al.: Submillisievert radiation dose coronary CT angiography: clinical impact of the knowledge-based iterative model reconstruction. Acad Radiol 2016; 23: pp. 1393-1401.
27. Nishiyama Y., Tada K., Mori H., et. al.: Effect of the forward-projected model-based iterative reconstruction solution algorithm on image quality and radiation dose in pediatric cardiac computed tomography. Pediatr Radiol 2016; 46: pp. 1663-1670.