
Rationale and Objectives
The aim of this study was to investigate whether a respiratory biofeedback system could increase navigator efficiency and maintain image quality compared to conventional respiratory-gated magnetic resonance coronary angiography (MRCA).
Materials and Methods
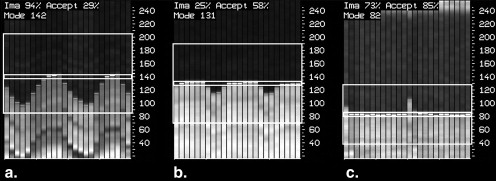
Eighteen healthy volunteers underwent MRCA using three different respiratory-gating protocols. A conventional expiratory free-breathing (FB) sequence was compared to two approaches using navigator echo biofeedback (NEB), a midinspiratory approach (NEBin) and an expiratory approach (NEBex). Navigator data reflecting the position of the diaphragm relative to a 3-mm gating window were made available to the subject using a video projector in combination with a Plexiglas screen and mirror goggles. Image quality was graded by two radiologists in consensus using a visual score ranging from 1 (not visible) to 4 (excellent vessel depiction).
Results
The NEB approaches improved navigator efficiency (71.1% with NEBex and 68.0% with NEBin vs 42.2% with FB), thus reducing total imaging time. This difference was statistically significant ( P NEBin = .007; P NEBex = .001). Image quality in the NEBex group was comparable to that in the FB group (median score, 2.44 vs 2.52), but it proved to be significantly lower (median score, 1.94 vs 2.52) for the right coronary artery and the left anterior descending coronary artery in the NEBin group.
Conclusion
NEB maintains image quality and significantly increases navigator efficiency, thereby decreasing total imaging time by about 40% compared to a conventional FB acquisition strategy.
The noninvasive nature of magnetic resonance coronary angiography (MRCA) offers great potential for assessing the morphologic changes in coronary artery disease (CAD) . The benefits of excluding CAD must be balanced against the risks and adverse effects of highly invasive procedures such as conventional catheter angiography, especially in patients with low pretest probability of disease.
The two main challenges that limit the introduction of MRCA into clinical routine are cardiac and respiratory motion that give rise to severe artifacts and blurring . Various strategies have been used to compensate for motion artifacts, including cardiac gating , respiratory gating , and navigator echoes with or without section correction. To reduce or eliminate respiratory motion artifacts, two distinct approaches are used in modern MRCA: using a navigator echo to measure the superior-inferior position of the diaphragm and accepting data acquired only in a certain range while the subject breathes freely . This is usually done at the most likely position of the diaphragm (ie, end-expiration).
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
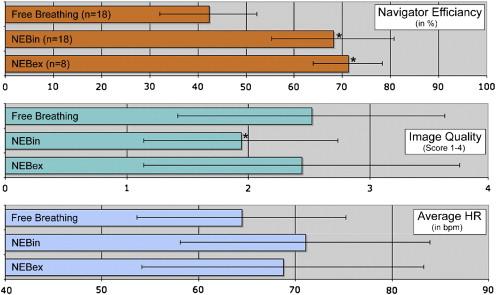
Table 1
Navigator Efficiency, Image Quality, and Heart Rate Data of the Three Study Groups
Navigator Technique_n_ Navigator Efficiency (%) Image Quality (Score 1–4) Average HR (beats/min) HR Variability (beats/min) Free breathing 18 42.2 ± 10.1 2.52 ± 1.1 64.4 ± 10.8 2.8 ± 1.5 NEBin 18 68.0 ∗ ± 12.7 1.94 ∗ ± 0.8 71.0 ± 12.9 3.8 ± 1.8 NEBex 8 71.1 ∗ ± 7.2 2.44 ± 1.3 68.7 ± 14.6 3.1 ± 1.4
HR, heart rate; NEBex, expiratory navigator echo biofeedback; NEBin, expiratory navigator echo biofeedback.
Data are expressed as mean ± standard deviation.
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Kim W.Y., Danias P.G., Stuber M., Flamm S.D., Plein S., Nagel E., et. al.: Coronary magnetic resonance angiography for the detection of coronary stenoses. N Engl J Med 2001; 345: pp. 1863-1869.
2. Manning W.J., Li W., Edelman R.R.: A preliminary report comparing magnetic resonance coronary angiography with conventional angiography. N Engl J Med 1993; 328: pp. 828-832.
3. Johnson K.R., Patel S.J., Whigham A., Hakim A., Pettigrew R.I., Oshinski J.N.: Three-dimensional, time-resolved motion of the coronary arteries. J Cardiovasc Magn Reson 2004; 6: pp. 663-673.
4. Wesbey G., Higgins C.B., Lanzer P., Botvinick E., Lipton M.J.: Imaging and characterization of acute myocardial infarction in vivo by gated nuclear magnetic resonance. Circulation 1984; 69: pp. 125-130.
5. Ehman R.L., McNamara M.T., Pallack M., Hricak H., Higgins C.B.: Magnetic resonance imaging with respiratory gating: techniques and advantages. AJR Am J Roentgenol 1984; 143: pp. 1175-1182.
6. Sachs T.S., Meyer C.H., Irarrazabal P., Hu B.S., Nishimura D.G., Macovski A.: The diminishing variance algorithm for real-time reduction of motion artifacts in MRI. Magn Reson Med 1995; 34: pp. 412-422.
7. Li D., Kaushikkar S., Haacke E.M., Woodard P.K., Dhawale P.J., Kroeker R.M., et. al.: Coronary arteries: three-dimensional MR imaging with retrospective respiratory gating. Radiology 1996; 201: pp. 857-863.
8. Edelman R.R., Manning W.J., Burstein D., Paulin S.: Coronary arteries: breath-hold MR angiography. Radiology 1991; 181: pp. 641-643.
9. Liu Y.L., Riederer S.J., Rossman P.J., Grimm R.C., Debbins J.P., Ehman R.L.: A monitoring, feedback, and triggering system for reproducible breath-hold MR imaging. Magn Reson Med 1993; 30: pp. 507-511.
10. Wang Y., Rossman P.J., Grimm R.C., Riederer S.J., Ehman R.L.: Navigator-echo-based real-time respiratory gating and triggering for reduction of respiration effects in three-dimensional coronary MR angiography. Radiology 1996; 198: pp. 55-60.
11. McCarthy R.M., Shea S.M., Deshpande V.S., Green J.D., Pereles F.S., Carr J.C., et. al.: Coronary MR angiography: true FISP imaging improved by prolonging breath holds with preoxygenation in healthy volunteers. Radiology 2003; 227: pp. 283-288.
12. Jahnke C., Paetsch I., Schnackenburg B., Bornstedt A., Gebker R., Fleck E., et. al.: Coronary MR angiography with steady-state free precession: individually adapted breath-hold technique versus free-breathing technique. Radiology 2004; 232: pp. 669-676.
13. Roussos C.: Function and fatigue of respiratory muscles. Chest 1985; 88: pp. 124S-132S.
14. Chung C.S., Karamanoglu M., Kovacs S.J.: Duration of diastole and its phases as a function of heart rate during supine bicycle exercise. Am J Physiol Heart Circ Physiol 2004; 287: pp. H2003-H2008.
15. Kovacs S.J.: The duration of the QT interval as a function of heart rate: a derivation based on physical principles and a comparison to measured values. Am Heart J 1985; 110: pp. 872-878.