
Rationale and Objectives
Cross-sectional imaging is being increasingly proposed as a suitable tool to characterize carotid plaques. The aim of this work was to correlate the Doppler velocity parameters with the cross-sectional percent stenosis (CPoS) of internal carotid artery (ICA) and to identify the cutoff values of these parameters in five progressive classes of stenosis area severity (ie, 40%–49%, 50%–59%, 60%–69%, 70%–79%, 80%–90%).
Materials and Methods
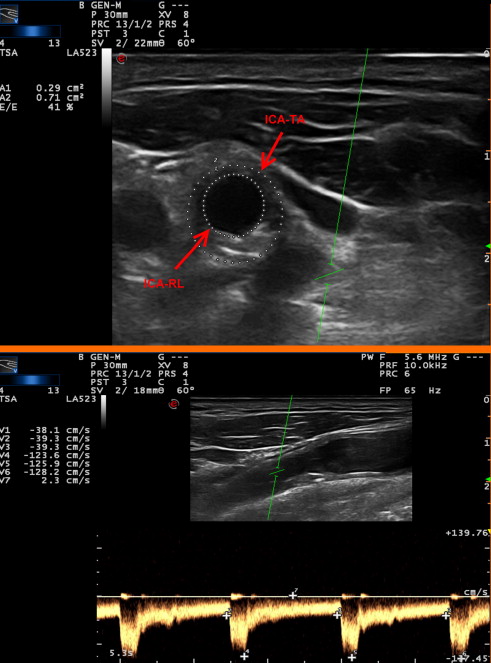
High-quality scans from 90 patients (mean age, 74 ± 9 years) with 43%–90% ICA stenosis were analyzed. ICA peak-systolic (PSV) and end-diastolic (EDV) velocities were measured at maximum stenosis level. Total ICA area and residual lumen (RL) were measured to derive the CPoS. A simple physical model described by the equation Velocity = Flow rate/Area was considered. Effectively, the CPoS is expected to negatively correlate with the inverse of velocity parameters, assuming flow rate to be constant. Multiple stepwise regression analyses were used to investigate the relationships between velocity and echographic measures.
Results
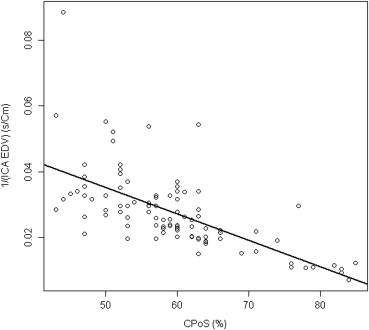
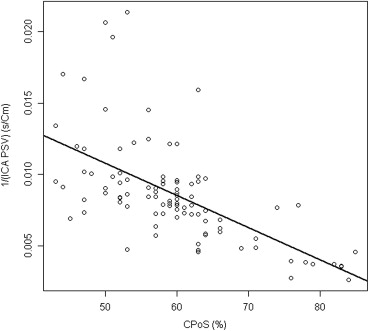
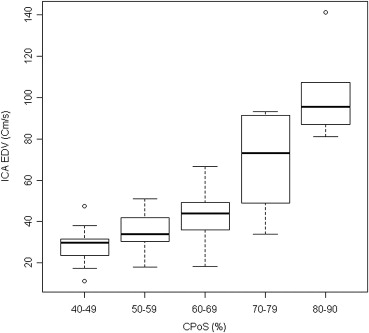
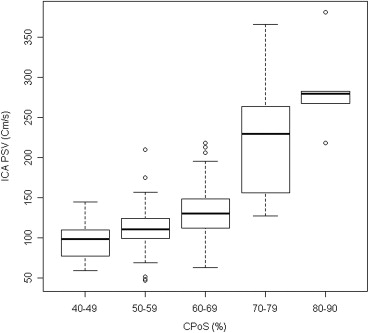
With CPoS as the dependent variable, the first significant regressor was the inverse ICA-EDV ( r 2 = 0.64; P < .0001) followed by inverse ICA-PSV ( r 2 = 0.43; P < .0001). ICA-EDV mean values throughout five progressive classes of stenosis were: 28 cm/second for 40%–49% stenosis, 35 cm/second for 50%–59%, 43 cm/second for 60%–69%, 69 cm/second for 70%–79%. and 103 cm/second for 80%–90%. ICA-PSV mean values were: 97 cm/second for 40%–49%, 110 cm/second for 50%–59%, 136 cm/second for 60%–69%, 224 cm/second for 70%–79%, and 286 cm/second for 80%–90%.
Conclusion
ICA-EDV is the parameter that better correlates with CPoS. Nevertheless, ICA-PSV maintained a highly significant correlation with CPoS. Moreover, the categorization of Doppler parameters in five progressive classes of severity of stenosis could provide physicians with an easily accessible tool in clinical practice, complementary to the morphological evaluation of cross-sectional stenosis.
Carotid stenosis is a target for stroke prevention interventions and potentially a target for population screening campaigns. Characterizing carotid stenosis is useful in risk stratification and is helpful in selecting the most appropriate risk-reducing interventions for individual patients. Medical intervention to reduce risk has become very effective ; hence, reproducible methods to characterize stenosis severity may help in monitoring the effectiveness of medical intervention. Therefore, it is crucial to evaluate methods to detect and characterize carotid plaques, including degree of stenosis in an accurate, reproducible, safe, and accessible way. Traditionally, the degree of stenosis in internal carotid artery (ICA) has been measured by means of conventional digital subtraction angiography (DSA). Today, the latter has been largely replaced by noninvasive tools, such as duplex ultrasound (DUS), minimally invasive computed tomography angiography (CTA), or magnetic resonance angiography (MRA) , because conventional angiography is relatively dangerous (eg, embolic risk, allergic reactions, retroperitoneal hemorrhage, groin hematoma), expensive, and relatively difficult to perform because of the limiting use to tertiary referral centers. Moreover, when using conventional angiography, degree of stenosis is defined by means of one to three longitudinal views of the lumen, which limits accuracy and reproducibility of the evaluation, and little information is provided about cross-sectional plaque characteristics. Actually, degree of stenosis was traditionally defined by using conventional angiography methods, mainly by means of NASCET (North American Symptomatic Carotid Endarterectomy Trial) and ECST (European Carotid Surgery Trial)-derived parameters . Several discrepancies have been shown between these two methods , generating confusion in the application of their recommendations to clinical practice . Furthermore, longitudinal measurements may lead to a suboptimal evaluation of the hemodynamic meaning of the stenosis, at least in those (not unusual) cases where sectional morphology of arteries with plaques is irregular . Therefore, cross-sectional area would be a more accurate parameter than longitudinal measurements to infer the real residual blood flow velocities through a stenosed artery , especially in evaluating those stenoses with a noncircular lumen . When properly validated, cross-sectional imaging might indeed replace the conventional gold standard to better characterize carotid plaque.
Indeed, when the plaque surface and/or vessel wall borders were well identifiable, DUS cross-sectional area evaluation could be a reliable tool in order to define the degree of ICA stenosis. This has been supported by gross pathological studies showing that cross-sectional area, even if measured by means of DUS, is more accurate than longitudinal measurements versus the gold standard of fixed histological endarterectomy specimens . Actually, DUS is the most widely used screening and diagnostic technique because of its limited cost and sufficient accuracy, especially for the detection of carotid bifurcation plaques . It is more accessible and less risky than contrast MRA and contrast CTA. Moreover, DUS is reliable in assessing stenosis . It is noninvasive, less expensive, and may be easily performed in an emergency setting .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Patients
Get Radiology Tree app to read full this article<
Sonographic Examinations
Get Radiology Tree app to read full this article<
CPoS=[(TA–RL)/TA]∗100 CPoS
=
[
(
TA
–
RL
)
/
TA
]
∗
100
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Regression Analysis between CPoS and the Inverse of Velocity Parameters
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Regression Analysis between CPoS, the Inverse of Velocity Parameters, and Native Echographic Measures
Get Radiology Tree app to read full this article<
Relationship between CPoS and ICA-EDV/ICA-PSV in Five Progressive Classes of Stenosis Severity
Get Radiology Tree app to read full this article<
Table 1
ICA-EDV and ICA-PSV Mean Values, Standard Deviation, and Standard Error within Five Classes of Degree of Stenosis
CPoS (%) EDV in ICA (cm/second) PSV in ICA (cm/second) Mean SD SE Mean SD SE 40–49 28 9 3 97 26 7 50–59 35 9 1 110 33 5 60–69 43 11 2 136 36 6 70–79 69 24 8 224 80 28 80–90 103 24 11 286 59 27
CPoS, cross-sectional percent stenosis; EDV, end-diastolic velocity; ICA, internal carotid artery; PSV, peak systolic velocity; SD, standard deviation; SE, standard error.
Get Radiology Tree app to read full this article<
Post-hoc Analysis
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Nicolaides A.N., Kakkos S.K., Kyriacou E., et. al.: Asymptomatic internal carotid artery stenosis and cerebrovascular risk stratification. J Vasc Surg 2010; 52: pp. 1486-1496. e1–e5
2. Abbott A.L.: Medical (nonsurgical) intervention alone is now best for prevention of stroke associated with asymptomatic severe carotid stenosis: results of a systematic review and analysis. Stroke 2009; 40: pp. e573-e583.
3. Naylor A.R., Gaines P.A., Rothwell P.M.: Who benefits most from intervention for asymptomatic carotid stenosis: patients or professionals?. Eur J Vasc Endovasc Surg 2009; 37: pp. 625-632.
4. Wardlaw J.M., Chappell F.M., Best J.J., et. al.: Non-invasive imaging compared with intra-arterial angiography in the diagnosis of symptomatic carotid stenosis: a meta-analysis. Lancet 2006; 367: pp. 1503-1512.
5. Staikov I.N., Arnold M., Mattle H.P., et. al.: Comparison of the ECST, CC, and NASCET grading methods and ultrasound for assessing carotid stenosis. European Carotid Surgery Trial. North American Symptomatic Carotid Endarterectomy Trial. J Neurol 2000; 247: pp. 681-686.
6. Nicolaides A.N., Shifrin E.G., Bradbury A., et. al.: Angiographic and duplex grading of internal carotid stenosis: can we overcome the confusion?. J Endovasc Surg 1996; 3: pp. 158-165.
7. Zhang Z., Berg M., Ikonen A., et. al.: Carotid stenosis degree in CT angiography: assessment based on luminal area versus luminal diameter measurements. Eur Radiol 2005; 15: pp. 2359-2565.
8. de Bray J.M., Glatt B.: Quantification of atheromatous stenosis in the extracranial internal carotid artery. Cerebrovasc Dis 1995; 5: pp. 414-426.
9. van Prehn J., Muhs B.E., Pramanik B., et. al.: Multidimensional characterization of carotid artery stenosis using CT imaging: a comparison with ultrasound grading and peak flow measurement. Eur J Vasc Endovasc Surg 2008; 36: pp. 267-272.
10. Porsche C., Walker L., Mendelow D., et. al.: Evaluation of cross-sectional luminal morphology in carotid atherosclerotic disease by use of spiral CT angiography. Stroke 2001; 32: pp. 2511-2515.
11. Jmor S., El-Atrozy T., Griffin M., et. al.: Grading internal carotid artery stenosis using B-mode ultrasound (in vivo study). Eur J Vasc Endovasc Surg 1999; 18: pp. 315-322.
12. Alexandrov A.V., Bladin C.F., Maggisano R., et. al.: Measuring carotid stenosis. Time for a reappraisal. Stroke 1993; 24: pp. 1292-1296.
13. Schulte-Altedorneburg G., Droste D.W., Felszeghy S., et. al.: Accuracy of in vivo carotid B-mode ultrasound compared with pathological analysis: intima-media thickening, lumen diameter, and cross-sectional area. Stroke 2001; 32: pp. 1520-1524.
14. Jaff M.R., Goldmakher G.V., Lev M.H., et. al.: Imaging of the carotid arteries: the role of duplex ultrasonography, magnetic resonance arteriography, and computerized tomographic arteriography. Vasc Med 2008; 13: pp. 281-292.
15. Bonig L., Weder B., Schott D., et. al.: Prediction of angiographic carotid artery stenosis indexes by colour Doppler-assisted duplex imaging. A critical appraisal of the parameters used. Eur J Neurol 2000; 7: pp. 183-190.
16. Scaroni R., Cardaioli G., Pelliccioli G.P., et. al.: Spiral computed tomography angiography (SCTA) and color coded duplex ultrasound (CCDUS): two complementary diagnostic techniques for assessment of extracranial cerebral artery stenosis. Clin Exp Hypertens 2002; 24: pp. 659-668.
17. Fell G., Phillips D.J., Chikos P.M., et. al.: Ultrasonic duplex scanning for disease of the carotid artery. Circulation 1981; 64: pp. 1191-1195.
18. Sabeti S., Schillinger M., Mlekusch W., et. al.: Quantification of internal carotid artery stenosis with duplex US: comparative analysis of different flow velocity criteria. Radiology 2004; 232: pp. 431-439.
19. Grant E.G., Benson C.B., Moneta G.L., et. al.: Carotid artery stenosis: gray-scale and Doppler US diagnosis—Society of Radiologists in Ultrasound Consensus Conference. Radiology 2003; 229: pp. 340-436.
20. Kochanowicz J., Turek G., Rutkowski R., et. al.: Normal reference values of ratios of blood flow velocities in internal carotid artery to those in common carotid artery using Doppler sonography. J Clin Ultrasound 2009; 37: pp. 208-211.
21. Braun R.M., Bertino R.E., Milbrandt J., et. al.: Ultrasound imaging of carotid artery stenosis: application of the Society of Radiologists in Ultrasound Consensus Criteria to a Single Institution Clinical Practice. Ultrasound Q 2008; 24: pp. 161-166.
22. Shaalan W.E., Wahlgren C.M., Desai T., et. al.: Reappraisal of velocity criteria for carotid bulb/internal carotid artery stenosis utilizing high-resolution B-mode ultrasound validated with computed tomography angiography. J Vasc Surg 2008; 48: pp. 104-112. discussion 112–113
23. Gaitini D., Soudack M.: Diagnosing carotid stenosis by Doppler sonography: state of the art. J Ultrasound Med 2005; 24: pp. 1127-1136.
24. R Development Core Team: R: A Language and Environment for Statistical Computing.2008.R Foundation for Statistical ComputingVienna, Austria
25. Faraway J. Practical Regression and Anova using R. Available at: http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.123.1025&rep=rep1&type=pdf . Accessed July, 2002.
26. Jahromi A.S., Cina C.S., Liu Y., et. al.: Sensitivity and specificity of color duplex ultrasound measurement in the estimation of internal carotid artery stenosis: a systematic review and meta-analysis. J Vasc Surg 2005; 41: pp. 962-972.
27. Arbeille P., Desombre C., Aesh B., et. al.: Quantification and assessment of carotid artery lesions: degree of stenosis and plaque volume. J Clin Ultrasound 1995; 23: pp. 113-124.
28. Benhamou A.C., Dutreix J.L., Genre O., et. al.: [Validation of quantitative and qualitative data of real-time carotid echotomography in comparison with standard Doppler tests, arteriography and anatomopathology. On 59 carotid endarterectomies]. J Mal Vasc 1984; 9: pp. 185-194.
29. Ricotta J.J., Bryan F.A., Bond M.G., et. al.: Multicenter validation study of real-time (B-mode) ultrasound, arteriography, and pathologic examination. J Vasc Surg 1987; 6: pp. 512-520.
30. Montorzi G., Silacci P., Zulliger M., et. al.: Functional, mechanical and geometrical adaptation of the arterial wall of a non-axisymmetric artery in vitro. J Hypertens 2004; 22: pp. 339-347.
31. Giannattasio C., Failla M., Emanuelli G., et. al.: Local effects of atherosclerotic plaque on arterial distensibility. Hypertension 2001; 38: pp. 1177-1180.
32. U-King-Im J.M., Young V., Gillard J.H.: Carotid-artery imaging in the diagnosis and management of patients at risk of stroke. Lancet Neurol 2009; 8: pp. 569-580.
33. Yazdani S.K., Vorpahl M., Ladich E., et. al.: Pathology and vulnerability of atherosclerotic plaque: identification, treatment options, and individual patient differences for prevention of stroke. Curr Treat Options Cardiovasc Med 2010; 12: pp. 297-314.
34. ten Kate G.L., Sijbrands E.J., Staub D., et. al.: Noninvasive imaging of the vulnerable atherosclerotic plaque. Curr Probl Cardiol 2010; 35: pp. 556-591.
35. Mathiesen E.B., Johnsen S.H.: Ultrasonographic measurements of subclinical carotid atherosclerosis in prediction of ischemic stroke. Acta Neurol Scand Suppl 2009; 189: pp. 68-72.
36. Wijeyaratne S.M., Jarvis S., Stead L.A., et. al.: A new method for characterizing carotid plaque: multiple cross-sectional view echomorphology. J Vasc Surg 2003; 37: pp. 778-784.
37. Makris G.C., Lavida A., Griffin M., et. al.: Three-dimensional ultrasound imaging for the evaluation of carotid atherosclerosis. Atherosclerosis 2011;
38. Vicenzini E., Galloni L., Ricciardi M.C., et. al.: Advantages and pitfalls of three-dimensional ultrasound imaging of carotid bifurcation. Eur Neurol 2011; 65: pp. 309-316.
39. de Labriolle A., Mohty D., Pacouret G., et. al.: Comparison of degree of stenosis and plaque volume for the assessment of carotid atherosclerosis using 2-D ultrasound. Ultrasound Med Biol 2009; 35: pp. 1436-1442.
40. Melissano G., Castellano R., Mazzitelli S., et. al.: Safe and cost-effective approach to carotid surgery. Eur J Vasc Endovasc Surg 1997; 14: pp. 164-169.
41. Ranaboldo C., Davies J., Chant A.: Duplex scanning alone before carotid endarterectomy: a 5-year experience. Eur J Vasc Surg 1991; 5: pp. 415-419.
42. Melissano G., Castellano R., Zucca R., et. al.: Results of carotid endarterectomy performed with preoperative duplex ultrasound assessment alone. Vasc Surg 2001; 35: pp. 95-101.