
Rationale and Objectives
To evaluate the clinical utility of cranial computed tomography (CT) in pediatric and adult patients during ongoing extracorporeal membrane oxygenation (ECMO) treatment from acute respiratory failure and to assess the frequency of intracranial hemorrhage (ICH) and infarction during the treatment.
Materials and Methods
The medical records of 123 consecutive patients, 54 children (ages 3 months–17 years) and 69 adults (ages 18–62 years), treated with ECMO over a 10-year period were searched for cranial CT performed during ECMO. Indications for CT, CT findings, impact on clinical management, and patient outcome were noted. In addition, all CT scans were reviewed for the frequency of ICH or infarction.
Results
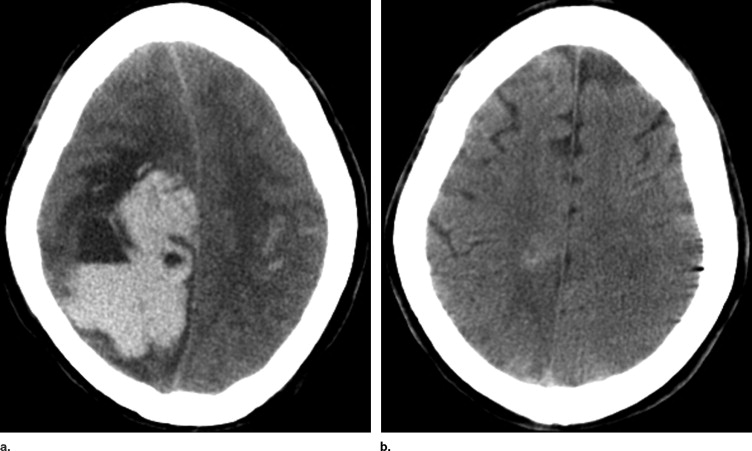
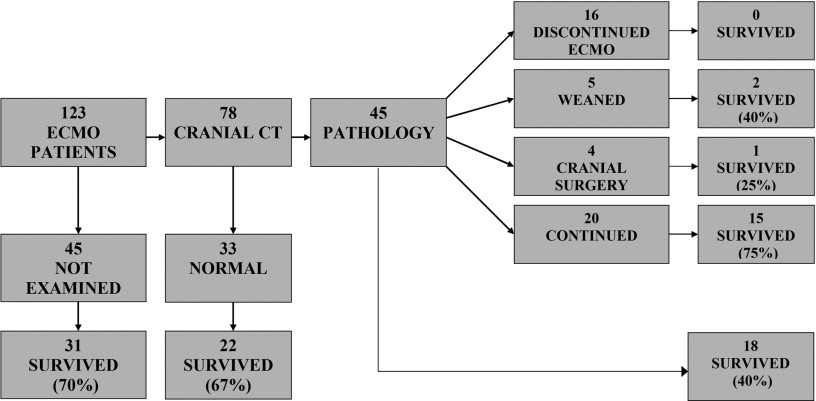
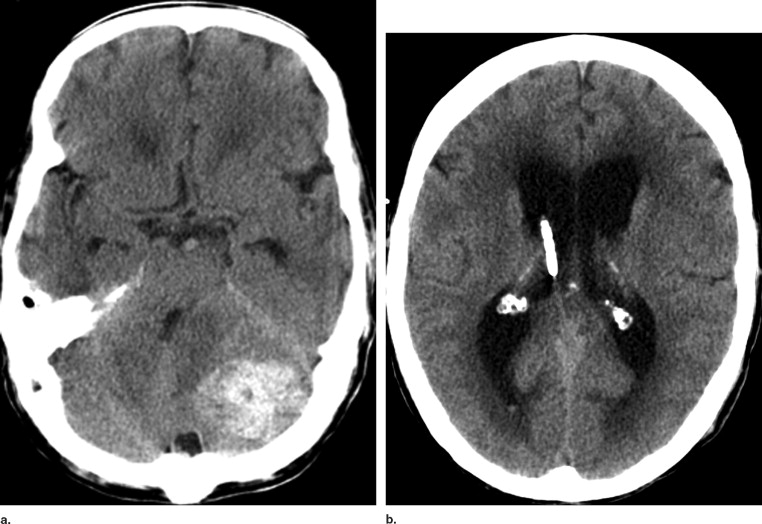
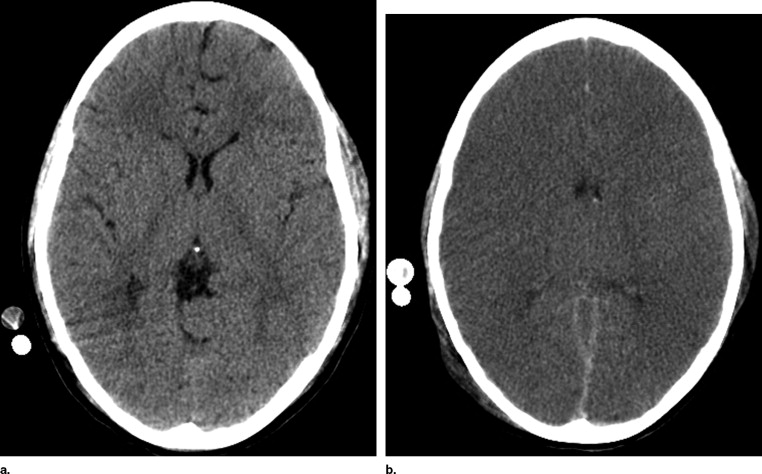
Seventy-eight patients had cranial CT while on ECMO. ICH or cerebral infarction were detected in 45 (37%) of the 123 patients. Eighteen patients (15%) had focal hemorrhage, 11 (9%) focal infarction, and 16 (13%) general brain edema. In 16 of the 45 patients, the CT findings were decisive to withdraw the ECMO treatment. Five patients were weaned from ECMO, and in four patients the findings motivated cranial surgery during ECMO. In the remaining 20 patients with less extended intracranial pathology, the ECMO treatment was continued with high survival.
Conclusion
Cranial CT has an important role during ECMO treatment to reveal or exclude severe intracranial complications where ECMO treatment should be discontinued. Less severe complications have a favorable prognosis with continued treatment. Our study suggests an underreporting of intracranial complications in adults and pediatric patients on ECMO because of low utilization of neuroimaging.
Extracorporeal membrane oxygenation (ECMO) is a commonly used therapy for neonates, children, and adults with acute, extremely severe respiratory failure unresponsive to conventional medical management and intensive care ( ). In randomized studies, ECMO has proved to be a life-saving technique in neonates with a number of pulmonary disorders ( ), and several nonrandomized investigations have shown promising results in children ( ) and adults ( ). By January 2006, more than 30,000 patients have been reported to the Extracorporeal Life Support Organization (ELSO) from approximately 100 ECMO centers ( ).
A significant cause of morbidity and mortality among patients on ECMO therapy are related to intracranial complications, mainly intracranial hemorrhage (ICH) and cerebral infarction ( ). This can be attributed to both pre-ECMO asphyxia or hypotension and to the ECMO procedure itself, including the altered blood flow after ligation of the internal jugular vein and common carotid artery and the increased risk for thromboembolism and hemorrhage from extracorporeal circulation, coagulopathy, and systemic heparinization.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Patients and Study Design
Get Radiology Tree app to read full this article<
Table 1
Descriptive Data for Pediatric and Adult Patients Treated With ECMO During the Study Period
Number ( n ) Age (Years) Mean (Range) Gender Diagnosis Cannulation Type Days on ECMO Mean (Range) Survival ( n ) Children 54 5.6 (0.25–17)
12.4 (0.5–49) 30 (56%) Adults 69 38 (18–62)
14.7 (0.1–59) 41 (59%) All 123 23.8 (0.25–62)
13.7 (0.1–59) 71 (58%)
ECMO: extracorporeal membrane oxygenation; F: female; M: male; ARDS: acute respiratory distress syndrome; ARF: acute respiratory failure; VA: veno-arterial; VV: veno-venous.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
ECMO Technique and Transports
Get Radiology Tree app to read full this article<
CT Examinations
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Ethics
Get Radiology Tree app to read full this article<
Results
CT Findings
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Intracranial Pathology in 45 Patients Diagnosed With Computed Tomography During Extracorporeal Membrane Oxygenation Treatment
Type of Intracranial Pathology_n_ Focal hemorrhage18 Supratentorial 11 Cerebellar 5 Extraaxial 2 Focal nonhemorrhagic infarction11 Supratentorial 10 Infratentorial 1 General edema/infarction16 Total45
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Effect on Treatment
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistics
Get Radiology Tree app to read full this article<
Table 3
Intracranial Pathology vs. Patient Characteristics Using the Chi-Square Test for Categorical and Student’s t -Test for Numerical Values
Patient Characteristics_P_ Value Age .43 Gender .78 Cannulation type .54 Days on extracorporeal membrane oxygenation .61 Diagnosis .06 Sepsis ⁎⁎ .004 ⁎ Survival .002 ⁎
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Frequency and Type of Intracranial Pathology
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Risk Factors for Intracranial Pathology
Get Radiology Tree app to read full this article<
Impact on Treatment
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Zwischenberger J.B., Bartlett R.H.: Extracorporeal life support: an overview.Van Meurs K.Lally K.P.Peek G. et. al.ECMO extracorporeal cardiopulmonary support in critical care.2005.Extracorporeal Life Support OrganizationAnn Arbor, MI:pp. 1-4.
2. Bartlett R.H., Roloff D.W., Custer J.R., et. al.: Extracorporeal life support. JAMA 2000; 283: pp. 904-908.
3. Bartlett R.H., Roloff D.W., Cornell R.G., et. al.: Extracorporeal circulation in neonatal respiratory failure: a prospective randomized study. Pediatrics 1985; 76: pp. 479-487.
4. UK Collaborative ECMO Trial Group: UK collaborative randomized trial of neonatal extracorporeal membrane oxygenation. Lancet 1996; 348: pp. 75-82.
5. Peek G.J., Sosnowski A.W.: Extra-corporeal membrane oxygenation for pediatric respiratory failure. Brit Med Bull 1997; 53: pp. 745-756.
6. Swaniker F., Kolla S., Moler F., et. al.: Extracorporeal life support outcome for 128 pediatric patients with respiratory failure. J Ped Surg 2000; 35: pp. 197-202.
7. Kolla S., Awad S.S., Rich P.B., et. al.: Extracorporeal life support for 100 adult patients with severe respiratory failure. Ann Surg 1997; 226: pp. 544-566.
8. Lewandowski K., Roissant R., Pappert D., et. al.: High survival rate in 122 ARDS patients managed according to a clinical algorithm including extracorporeal membrane oxygenation. Int Care Med 1997; 23: pp. 819-835.
9. Lindén V., Palmér K., Reinhard J., et. al.: High survival in adult patients with acute respiratory distress syndrome treated by extracorporeal membrane oxygenation, minimal sedation, and pressure supported ventilation. Int Care Med 2000; 26: pp. 1630-1637.
10. Extracorporeal Life Support Organization: 2006.Extracorporeal Life Support OrganizationAnn Arbor, MI
11. De Berry B.B., Lynch J., Chung D.H., et. al.: Emergencies during ECLS and their management.Van Meurs K.Lally K.P.Peek G. et. al.ECMO extracorporeal cardiopulmonary support in critical care.2005.Extracorporeal Life Support OrganizationAnn Arbor, MI:pp. 133-156.
12. Taylor G.A., Fitz C.R., Miller M.K., et. al.: Intracranial abnormalities in infants treated with extracorporeal membrane oxygenation: Imaging with US and CT. Radiology 1987; 165: pp. 675-678.
13. Babcock D.S., Kim Han B., Weiss R.G., et. al.: Brain abnormalities in infants on extracorporeal membrane oxygenation: sonographic and CT findings. AJR Am J Roentgenol 1989; 153: pp. 571-576.
14. Lazar E.L., Abramson S.J., Weinstein S., et. al.: Neuroimaging of brain injury in neonates treated with extracorporeal membrane oxygenation: lessons learned from serial examinations. J Ped Surg 1994; 29: pp. 86-191.
15. Bulas D.I., Taylor G.A., O’Donnell R.M., et. al.: Intracranial abnormalities in infants treated with extracorporeal membrane oxygenation: update on Sonographic and CT findings. AJNR 1996; 17: pp. 287-294.
16. Dalton H.J., Day S.E.: Neurologic outcome following ECLS in pediatric patients with respiratory or cardiac failure.Van Meurs K.Lally K.P.Peek G. et. al.ECMO extracorporeal cardiopulmonary support in critical care.2005.Extracorporeal Life Support OrganizationAnn Arbor, MI:pp. 383-392.
17. Amigoni A., Pettenazzo A., Biban P., et. al.: Neurologic outcome in children after extracorporeal membrane oxygenation: prognostic value of diagnostic tests. Pediatr Neurol 2005; 32: pp. 173-179.
18. Kasirajan V., Smedira N.G., McCarthy J.F., et. al.: Risk factors for intracranial hemorrhage in adults on extracorporeal membrane oxygenation. Eur J Cardiothor Surg 1999; 15: pp. 508-514.
19. Lidegran M., Palmér K., Jorulf H., et. al.: CT in the evaluation of patients on ECMO due to acute respiratory failure. Pediatr Radiol 2002; 32: pp. 567-574.
20. Lidegran M.K., Ringertz H.G., Frenckner B.P., et. al.: Chest and abdominal CT during extracorporeal membrane oxygenation: clinical benefits in diagnosis and treatment. Acad Radiol 2005; 12: pp. 276-285.
21. Lindén V., Palmér K., Reinhard J., et. al.: Inter-hospital transportation of patients with severe acute respiratory failure on extracorporeal membrane oxygenation—national and international experience. Int Care Med 2001; 27: pp. 1643-1648.
22. Horan M., Ichiba S., Firmin R.K., et. al.: A pilot investigation of mild hypothermia in neonates receiving extracorporeal membrane oxygenation (ECMO). J Pediatr 2004; 144: pp. 301-308.
23. Biehl D.A., Stewart D.L., Fort N.H., et. al.: Timing of intracranial hemorrhage during extracorporeal life support. ASAIO J 1996; 42: pp. 938-941.
24. Mendoza J.C., Shearer L.L., Cook L.M.: Lateralization of brain lesions following extracorporeal membrane oxygenation. Pediatrics 1991; 88: pp. 1004-1009.
25. Bulas D.I., Glass P., O’Donnell R.M., et. al.: Neonates treated with ECMO: predictive value of early CT and US neuroimaging findings on short-term neurodevelopmental outcome. Radiology 1995; 195: pp. 407-412.
26. Adolph V., Ekelund C., Smith C., et. al.: Developmental outcome of neonates treated with extracorporeal membrane oxygenation. J Pediatr Surg 1990; 25: pp. 43-46.
27. Brunberg J.A., Kewitz G., Schumacher R.E.: Venovenous extracorporeal membrane oxygenation: early CT alterations following use in management of severe respiratory failure in neonates. AJNR 1993; 14: pp. 595-603.
28. Hund E.: Critical illness polyneuropathy. Curr Opin Neurol 2001; 14: pp. 649-653.
29. Bartlett R.H., Chapman R.A.: Economics of ECLS.Van Meurs K.Lally K.P.Peek G. et. al.ECMO extracorporeal cardiopulmonary support in critical care.2005.Extracorporeal Life Support OrganizationAnn Arbor, MI:pp. 203-215.