
Rationale and Objectives
Historically, skills training in performing brain ultrasonography has been limited to hours of scanning infants for lack of adequate synthetic models or alternatives. The aim of this study was to create a simulator and determine its utility as an educational tool in teaching the skills that can be used in performing brain ultrasonography on infants.
Materials and Methods
A brain ultrasonography simulator was created using a combination of multi-modality imaging, three-dimensional printing, material and acoustic engineering, and sculpting and molding. Radiology residents participated prior to their pediatric rotation. The study included (1) an initial questionnaire and resident creation of three coronal images using the simulator; (2) brain ultrasonography lecture; (3) hands-on simulator practice; and (4) a follow-up questionnaire and re-creation of the same three coronal images on the simulator. A blinded radiologist scored the quality of the pre- and post-training images using metrics including symmetry of the images and inclusion of predetermined landmarks. Wilcoxon rank-sum test was used to compare pre- and post-training questionnaire rankings and image quality scores.
Results
Ten residents participated in the study. Analysis of pre- and post-training rankings showed improvements in technical knowledge and confidence, and reduction in anxiety in performing brain ultrasonography. Objective measures of image quality likewise improved. Mean reported value score for simulator training was high across participants who reported perceived improvements in scanning skills and enjoyment from simulator use, with interest in additional practice on the simulator and recommendations for its use.
Conclusions
This pilot study supports the use of a simulator in teaching radiology residents the skills that can be used to perform brain ultrasonography.
Introduction
Brain ultrasonography is a study frequently performed on neonates. In 2015 alone, 1459 such studies were performed at our tertiary-care children’s hospital, with the most common indications being a drop in hematocrit, enlarging anterior fontanelle, prematurity, pre- and peri-extracorporeal membrane oxygenation evaluations, and abnormal neurologic examination. Most of these studies were requested on an emergent basis, and they often play an essential role in guiding management . Given the ubiquity, time sensitivity, and importance of this examination, brain ultrasonography is a technique radiology trainees are expected to learn during residency training . However, most graduating residents are not proficient in performing this type of examination. The lack of supervision, structure, and assessment of competency during training had been cited as potential causes of this inadequacy . Additional pediatric radiology fellowship training is often required to attain proficiency.
Historically, brain ultrasonography is taught through a “master-apprentice” educational model in which an experienced provider performs the examination as the trainee observes. The trainee then attempts to perform the test under close supervision, slowly gaining the necessary psychomotor skills required to successfully perform the task . This approach has several drawbacks, including longer imaging times, patient discomfort/inconvenience/medical fragility, limited accessibility of patients, and risk of a suboptimal examination. In an increasingly demanding and time-constrained healthcare environment, opportunities for consistent trainee supervision and effective learning are becoming fewer and far between, further compromising this traditional master-apprentice educational model. Other medical fields that require skills training are faced with similar challenges and have turned to simulation training with varying degrees of success .
Get Radiology Tree app to read full this article<
Materials and Methods
Get Radiology Tree app to read full this article<
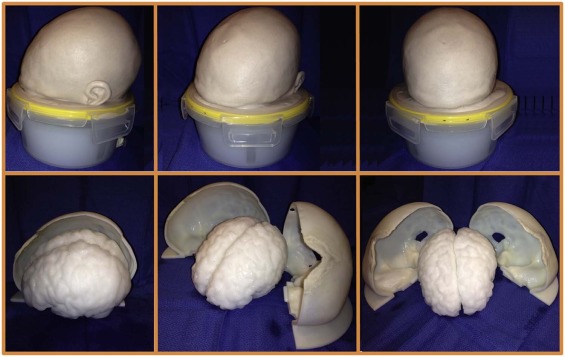
Construction of Simulator Model
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Brain Phantom
Get Radiology Tree app to read full this article<
Plastic Skull
Get Radiology Tree app to read full this article<
Skin Cover
Get Radiology Tree app to read full this article<
Assembly Process
Get Radiology Tree app to read full this article<
Study Participants
Get Radiology Tree app to read full this article<
Structure of Training Session
Get Radiology Tree app to read full this article<
Primer
Get Radiology Tree app to read full this article<
Pre-training Assessment
Get Radiology Tree app to read full this article<
Initial questionnaire
Get Radiology Tree app to read full this article<
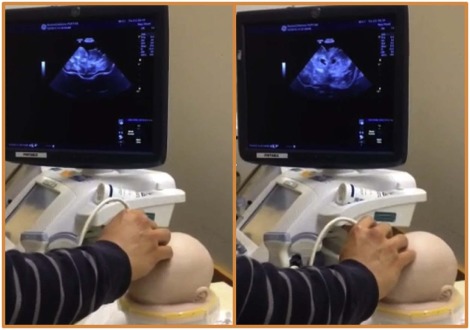
Creation of ultrasound images using the simulator
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Didactic Lecture
Get Radiology Tree app to read full this article<
Hands-on Simulator Practice
Get Radiology Tree app to read full this article<
Post-training Assessment
Get Radiology Tree app to read full this article<
Follow-up questionnaire
Get Radiology Tree app to read full this article<
Re-creation of ultrasound images using the simulator
Get Radiology Tree app to read full this article<
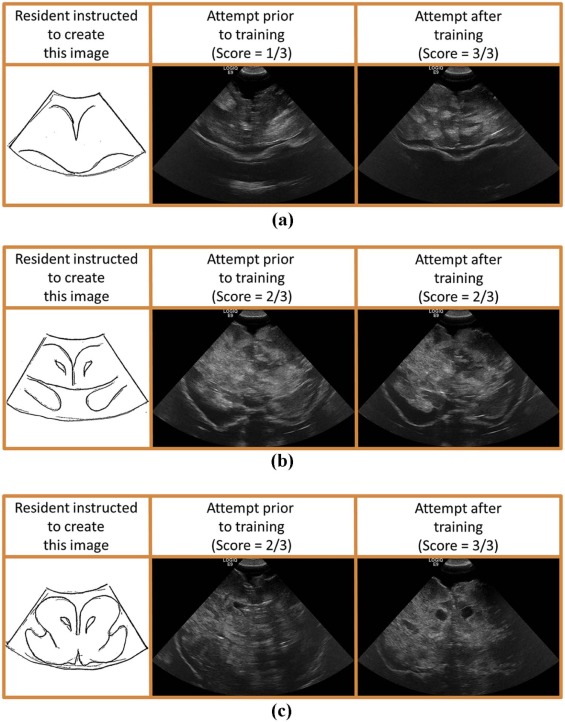
Image Quality Scoring
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Participant Demographics
Get Radiology Tree app to read full this article<
Pre- and Post-training Questionnaires
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Image Quality
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Completion Time
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Haber K., Wachter R.D., Christenson P.C., et. al.: Ultrasonic evaluation of intracranial pathology in infants: a new technique. Radiology 1980; 134: pp. 173-178.
2. London D.A., Carroll B.A., Enzmann D.R.: Sonography of ventricular size and germinal matrix hemorrhage in premature infants. AJR Am J Roentgenol 1980; 135: pp. 559-564.
3. Babcock D.S., Han B.K.: The accuracy of high resolution real-time ultrasonography of the head in infancy. Radiology 1981; 139: pp. 665-676.
4. Edwards M.K., Brown D.L., Muller J., et. al.: Cribside neurosonography: real-time sonography for intracranial investigation of the neonate. AJR Am J Roentgenol 1981; 136: pp. 271-275.
5. Grant E.G., Schellinger D., Borts F.T., et. al.: Real-time sonography of the neonatal and infant head. AJR Am J Roentgenol 1981; 136: pp. 265-270.
6. Pape K.E., Blackwell R.J., Cusick G., et. al.: Ultrasound detection of brain damage in preterm infants. Lancet 1979; 1: pp. 1261-1264.
7. Levene M.I., Wigglesworth J.S., Dubowitz V.: Cerebral structure and intraventricular haemorrhage in the neonate: a real-time ultrasound study. Arch Dis Child 1981; 56: pp. 416-424.
8. Mercuri E., Dubowitz L., Paterson Brown S., et. al.: Incidence of cranial ultrasound abnormalities in apparently well neonates on a postnatal ward: correlation with antenatal and perinatal factors and neurological status. Arch Dis Child Fetal Neonatal Ed 1998; 79: pp. F185-F189.
9. Dubinsky T.J., Garra B.S., Reading C., et. al.: Society of radiologists in ultrasound resident curriculum. Ultrasound Q 2013; 29: pp. 275-291.
10. Education Board of the Faculty of Clinical Radiology, The Royal College of Radiologists, 38 Portland Place, London W1N 4JQ : Core training: core skills in paediatrics.Structured training in clinical radiology.2001.Royal College of RadiologistsLondon: Available at www.rcr.ac.uk
11. Davis P.J., Cox R.M., Brooks J.: Training in neonatal cranial ultrasound: a questionnaire survey. Br J Radiol 2005; 78: pp. 55-56.
12. Nicholls D., Sweet L., Hyett J.: Psychomotor skills in medical ultrasound imaging: an analysis of the core skill set. J Ultrasound Med 2014; 33: pp. 1349-1352.
13. Waran V., Narayanan V., Karuppiah R., et. al.: Utility of multimaterial 3D printers in creating models with pathological entities to enhance the training experience of neurosurgeons. J Neurosurg 2014; 120: pp. 489-492.
14. Jacobsen M.D., Anderson M.J., Hansen C.O., et. al.: Testing basic competency in knee arthroscopy using a virtual reality simulator. J Bone Joint Surg Am 2015; 97: pp. 775-781.
15. Coughlin R.P., Pauyo T., Sutton J.C., et. al.: A validated orthopaedic surgical simulation model for training and evaluation of basic arthroscopic skills. J Bone Joint Surg Am 2015; 97: pp. 1465-1471.
16. Latif R.K., Bautista A., Duan X., et. al.: Teaching basic fiberoptic intubation skills in a simulator: initial learning and skills decay. J Anesth 2016; 30: pp. 12-19.
17. Cook D.A., Hatala R., Brydges R., et. al.: Technology-enhanced simulation for health professions education: a systematic review and meta-analysis. JAMA 2011; 306: pp. 978-988.
18. Surry K.J., Austin H.J., Fenster A., et. al.: Polyvinyl alcohol cryogel phantoms for use in ultrasound and MR imaging. Phys Med Biol 2004; 49: pp. 5529-5546.
19. Shadish W.R., Cook T.D., Campbell D.T.: Experimental and quasi-experimental designs for generalized causal inference.2002.Houghton Mifflin CompanyBoston, MA
20. Clark E.G., Paparello J.J., Wayne D.B., et. al.: Use of a national continuing medical education meeting to provide simulation-based training in temporary hemodialysis catheter insertion skills: a pre-test post-test study. Can J Kidney Health Dis 2014; 1: pp. 25-32.
21. Heiner J.D., McArthur T.J.: A simulation model for the ultrasound diagnosis of long-bone fractures. Simul Healthc 2009; 4: pp. 228-231.
22. Heiner J.D.: A new simulation model for skin abscess identification and management. Simul Healthc 2010; 5: pp. 238-241.
23. Zerth H., Harwood R., Tommaso L., et. al.: An inexpensive, easily constructed, reusable task trainer for simulating ultrasound-guided pericardiocentesis. J Emerg Med 2012; 43: pp. 1066-1069.
24. Sekhar A., Sun M.R., Siewert B.: A tissue phantom model for training residents in ultrasound-guided liver biopsy. Acad Radiol 2014; 21: pp. 902-908.
25. Akoma U.N., Shumard K.M., Street L., et. al.: Impact of an inexpensive anatomy-based fetal pig simulator on obstetric ultrasound training. J Ultrasound Med 2015; 34: pp. 1793-1799.
26. Morrow D.S., Broder J.: Cost-effective, reusable, leak-resistant ultrasound-guided vascular access trainer. J Emerg Med 2015; 49: pp. 313-317.
27. Shumard K.M., Akoma U.N., Street L.M., et. al.: Development of a novel task trainer for second trimester ultrasound-guided uterine evacuation. Simul Healthc 2015; 10: pp. 49-53.
28. Rudolph J.W., Simon R., Raemer D.B.: Which reality matters? Questions on the path to high engagement in healthcare simulation. Simul Healthc 2007; 2: pp. 161-163.
29. Matsumoto E.D., Hamstra S.J., Radomski S.B., et. al.: The effect of bench model fidelity on endourological skills: a randomized controlled study. J Urol 2002; 167: pp. 1243-1247.