
Rationale and Objectives
Cancer of the kidney is the third most common cancer of the urinary tract, and renal cell carcinoma is the most lethal of all genitourinary tumors. The incidental discovery of renal cell carcinoma has increased with increased use of cross-sectional imaging. Concomitantly, minimally invasive ablative technologies, including image-guided cryoablation, radiofrequency ablation, and others, have evolved as therapeutic options for small renal masses.
Materials and Methods
Between 2006 and 2009, 111 patients (age range, 31–91 years; mean age, 70 years) underwent percutaneous computed tomography–guided thermal ablation for suspected renal cell carcinoma at two major academic centers. Outcomes data were retrospectively collected and analyzed to compare recurrence rates for patients undergoing radiofrequency ablation ( n = 41) versus cryoablation ( n = 70).
Results
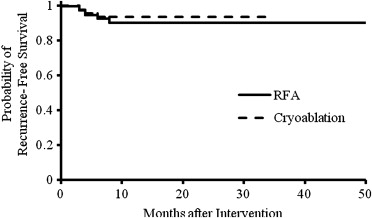
There were four cases of suspicious enhancement on follow-up computed tomography or magnetic resonance imaging in each group, with cumulative imaging recurrence rates of 11% and 7% for radiofrequency ablation and cryoablation, respectively. Log rank test analysis revealed no significant difference between rates of imaging recurrence between the two groups ( P = .6044).
Conclusions
These results suggest that the use of cryoablative technology will result in similar outcomes compared with radiofrequency ablation.
Accounting for 3.5% of all malignancies, cancer of the kidney is the third most common cancer of the urinary tract behind prostate cancer and transitional cell carcinoma of the urinary bladder . There were an estimated 58,000 new cases of renal cell carcinoma in 2009, with 13,000 deaths attributable to the disease, manifesting as the most lethal of all genitourinary tumors. The incidental discovery of renal cell carcinoma has risen dramatically during recent years because of the increased use of cross-sectional imaging . During the same time, minimally invasive techniques have evolved from nephron-sparing laparoscopic techniques to percutaneous image-guided ablations. For small renal masses (SRMs; <3 cm), percutaneous ablation guided by computed tomography (CT) or magnetic resonance imaging (MRI) is becoming the standard of care .
Concomitant with this evolution, multiple ablative modalities have become available, including radiofrequency ablation (RFA), cryoablation, percutaneous ethanol instillation, microwave, ultrasound, and more. A large body of literature is accumulating, composed of reports and single-arm series of percutaneous ablations in this setting . RFA and cryoablation are the two most commonly used techniques. To our knowledge, however, no comparative reports have been generated thus far.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Distribution of Histologic Review of Ablated Lesions
Clear Cell Renal Cell Carcinoma Papillary Type Renal Cell Carcinoma Oncocytoma Angiomyolipoma Insufficient Tissue for Definitive Diagnosis 74 (67%) 18 (16%) 9 (8%) 4 (4%) 6 (6%)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Summary of Collected Data and Rate of Recurrence for RFA and Cryoablation of Small Renal Masses
Variable RFA Cryoablation Number of cases 41 70 Suspicious enhancement on follow-up 4 4 Recurrence confirmed on histologic biopsy 0 0 Estimated imaging recurrence at 10 months 11% 7%
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<


Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Jemal A., Siegel R., Ward E., et. al.: Cancer statistics, 2009. CA Cancer J Clin 2009; 59: pp. 225-249.
2. Chawla S.N., Crispen P.L., Hanlon A.L., et. al.: The natural history of observed enhancing renal masses: meta-analysis and review of the world literature. J Urol 2006; 175: pp. 425-431.
3. Jayson M., Sanders H.: Increased incidence of serendipitously discovered renal cell carcinoma. Urology 1998; 51: pp. 203-205.
4. Volpe A., Panzarella T., Rendon R.A., et. al.: The natural history of incidentally detected small renal masses. Cancer 2004; 100: pp. 738-745.
5. Uppot R.N., Silverman S.G., Zagoria R.J., Tuncali K., et. al.: Imaging-guided percutaneous ablation of renal cell carcinoma: a primer of how we do it. AJR Am J Roentgenol 2009; 192: pp. 1558-1570.
6. Gill I.S., Aron M., Gervais D.A., et. al.: Small renal mass. N Engl J Med 2010; 362: pp. 624-634.
7. Littrup P.J., Ahmed A., Aoun H.D., et. al.: CT-guided percutaneous cryotherapy of renal masses. J Vasc Interv Radiol 2007; 18: pp. 383-392.
8. Kutikov A., Kunkle D.A., Uzzo R.G.: Focal therapy for kidney and prostate cancer. Curr Opin Urol 2009; 19: pp. 148-153.
9. Schmit G.D., Atwell T.D., Callstrom M.R.: Percutaneous cryoablation of renal masses >or=3 cm: efficacy and safety in treatment of 108 patients. J Endourol 2010; 24: pp. 1255-1262.
10. Autorino R., Haber G.P., White M.A., et. al.: New developments in renal focal therapy. J Endourol 2010; 24: pp. 665-672.
11. del Cura J.L., Zabala R., Iriarte J.I., et. al.: Treatment of renal tumors by percutaneous ultrasound guided radiofrequency ablation using a multitined electrode: effectiveness and complications. Eur Urol 2010; 57: pp. 459-465.
12. Silverman S.G., Tuncali K., vanSonnenberg , et. al.: Renal tumors: MR imaging-guided percutaneous cryotherapy-initial experience in 23 patients. Radiology 2005; 236: pp. 716-724.
13. Goldberg S.N., Grassi C.J., Cardella J.F., et. al.: Image guided tumor ablation: standardization of terminology and reporting criteria. Radiology 2005; 235: pp. 728-739.
14. Gill I.S., Remer E.M., Hasan W.A., et. al.: Renal cryoablation: outcome at 3 years. J Urol 2005; 173: pp. 1903-1907.
15. Zagoria R.J., Traver M.A., Werle D.M., et. al.: Oncologic efficacy of CT guided percutaneous radiofrequency ablation of renal cell carcinomas. AJR Am J Roentgenol 2007; 189: pp. 429-436.
16. Breen D.J., Rutherford E.E., Stedman B., et. al.: Management of renal tumors by image-guided radiofrequency ablation: experience in 105 tumors. Cardiovasc Intervent Radiol 2007; 30: pp. 936-942.
17. Gervais D.A., McGovern F.J., Arellano R.S., McDougal W.S., et. al.: Radiofrequency ablation of renal cell carcinoma. Part 1. Indications, results, and role in patient management over a 6-year period and ablation of 100 tumors. AJR Am J Roentgenol 2005; 185: pp. 64-71.
18. Gervais D.A., Arellano R.S., McGovern F.J., McDougal W.S., et. al.: Radiofrequency ablation of renal cell carcinoma. Part 2. Lessons learned with ablation of 100 tumors. AJR Am J Roentgenol 2005; 185: pp. 72-80.
19. Iang P., Wang Y., Zhang D., et. al.: Ultrasound guided percutaneous microwave ablation for small renal cancer: initial experience. J Urol 2008; 180: pp. 844-848.
20. Hafron J., Kaouk J.H.: Ablative techniques for the management of kidney cancer. Nat Clin Pract Urol 2007; 4: pp. 261-269.
21. Zlotta A.R., Wildschutz T., Raviv G., et. al.: Radiofrequency interstitial tumor ablation (RITA) is a possible new modality for treatment of renal cancer: ex vivo and in vivo experience. J Endourol 1997; 11: pp. 251-258.
22. McGovern F.J., Wood B.J., Goldberg S.N., et. al.: Radio frequency ablation of renal cell carcinoma via image guided needle electrodes. J Urol 1999; 161: pp. 599-600.
23. Aron M., Gill I.S.: Minimally invasive nephron-sparing surgery (MINSS) for renal tumours. Part II: probe ablative therapy. Eur Urol 2007; 51: pp. 348-357.
24. Goldberg S.N., Gazelle G.S., Mueller P.R.: Thermal ablation therapy for focal malignancy: a unified approach to underlying principles, techniques, and diagnostic imaging guidance. AJR Am J Roentgenol 2000; 174: pp. 323-331.
25. Uchida M., Imaide Y., Sugimoto K., et. al.: Percutaneous cryosurgery for renal tumours. Br J Urol 1995; 75: pp. 132-136.
26. Onik G.M., Reyes G., Cohen J.K., et. al.: Ultrasound characteristics of renal cryosurgery. Urology 1993; 42: pp. 212-215.
27. Hoffmann N.E., Bischof J.C.: The cryobiology of cryosurgical injury. Urology 2002; 60: pp. 40-49.
28. Kunkle D.A., Uzzo R.G.: Cryoablation or radiofrequency ablation of the small renal mass, a meta-analysis. Cancer 2008; 113: pp. 2671-2680.
29. Pahernik S., Ziegler S., Roos F., et. al.: Small renal tumors: correlation of clinical and pathological features with tumor size. J Urol 2007; 178: pp. 414-417.
30. Soldevilla J.I., de la Illa N.S., Viscasillas I.L., et. al.: Current treatment of small renal masses. Actas Urologicas Espanolas 2009; 33: pp. 505-513.
31. Remzi M., Ozsoy M., Klingler H.C., et. al.: Are small renal tumors harmless? Analysis of histopathological features according to tumors 4cm or less in diameter. J Urol 2006; 176: pp. 896-899.
32. Raman J.D., Hall D.W., Cadeddu J.A.: Renal ablative therapy: radiofrequency ablation and cryoablation. J Surg Oncol 2009; 100: pp. 639-644.
33. Aron M., Gill I.S.: Renal tumor ablation. Curr Opin Urol 2005; 15: pp. 298-305.
34. Kwan K.G., Matsumoto E.D.: Radiofrequency ablation and cryoablation of renal tumours. Curr Oncol 2007; 14: pp. 34-38.
35. Lehman D.S., Landman J.: Kidney cancer ablative therapy: indications and patient selection. Curr Urol Rep 2008; 9: pp. 34-43.
36. Lehman D.S., Landman J.: Cryoablation and radiofrequency for kidney tumor. Curr Urol Rep 2008; 9: pp. 128-134.
37. Pinkhasov GI, Raman JD. Management and prevention of renal ablative therapy complications. World J Urol Web. In press.
38. Johnson D.B., Solomon S.B., Su L.M., et. al.: Defining the complications of cryoablation and radio frequency ablation of small renal tumors: a multi-institutional review. J Urol 2004; 172: pp. 874-877.