
Rationale and Objectives
This study aims to compare the diagnostic performance of abdominal computed tomography (CT) performed with and without oral contrast in patients presenting to the emergency department (ED) with acute nontraumatic abdominal pain.
Materials and Methods
Between December 2013 and December 2014, 348 adult patients presenting to the ED of a large tertiary medical center with nontraumatic abdominal pain were evaluated. Exclusion criteria for the study were history of inflammatory bowel disease, recent abdominal operation and suspected renal colic, abdominal aortic aneurysm rupture, or intestinal obstruction. All patients underwent intravenous contrast-enhanced abdominal CT on a Philips Brilliance 64-slice scanner using a routine abdomen protocol. The study group included 174 patients who underwent abdominal CT scanning without oral contrast, recruited using convenience sampling. A control group of 174 patients was matched to the cohort groups’ gender and age and underwent abdominal CT with oral contrast material during the same time period. The patients’ medical records were reviewed for various clinical findings and for the final clinical diagnosis. The CT exams were initially reviewed by a senior attending radiologist to determine the exams’ technical adequacy and to decide whether an additional scan with oral contrast was required. Two senior radiologists, blinded to the clinical diagnosis, later performed consensus reading to determine the contribution of oral contrast administration to the radiologists’ diagnostic confidence and its influence on diagnosing various radiological findings.
Results
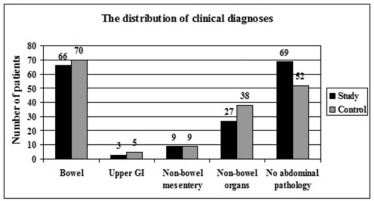
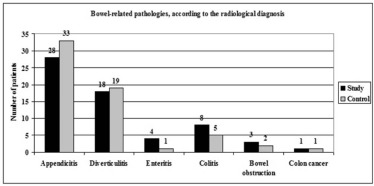
Each group consisted of 82 men and 92 women. The average age of the two groups was 48 years. The main clinical diagnoses of the pathological examinations were appendicitis (17.5%), diverticulitis (10.9%), and colitis (5.2%). A normal CT examination was found in 34.8% of the patients. There was no significant difference between the groups regarding most of the clinical parameters that were examined. None of the examinations of all of the 174 study group patients was found to be technically inadequate, and therefore no patient had to undergo additional scanning to establish a diagnosis. The consensus reading of the senior radiologists determined that the lack of oral contrast was insignificant in 96.6% of the cases and that contrast material might have been useful in only 6 of 174 study group patients (3.4%). The radiologists found oral contrast to be helpful only in 8 of 174 control group patients (4.6%). There was no significant difference between the clinical and radiological diagnoses in both groups (study group, P = 0.261; control group, P = 0.075).
Conclusions
Our study shows that oral contrast is noncontributory to radiological diagnosis in most patients presenting to the ED with acute nontraumatic abdominal pain. These patients can therefore undergo abdominal CT scanning without oral contrast, with no effect on radiological diagnostic performance.
Introduction
Computed tomography (CT) is the imaging modality of choice for the diagnosis of many causes of acute abdominal pain. CT protocols for evaluating patients presenting with acute nontraumatic abdominal pain commonly include the use of oral and intravenous (IV) contrast agents. This widely used protocol is considered to provide the most diagnostic information but is based on data from the earliest days of abdominal CT imaging. The introduction of helical and multidetector CT scanners has made the utility of oral contrast uncertain. The use of both oral and IV contrast materials is remarkably sensitive and specific for the diagnosis of bowel-related pathologies, but is not necessarily the most efficient and safe protocol . There are no formal definite guidelines regarding the optimal use of oral contrast in patients presenting to the emergency department (ED) with acute nontraumatic abdominal pain, and this has led to a wide variation in clinical practice .
The use of oral contrast material for abdominal CT examinations may have several disadvantages, including potential adverse effects of the oral contrast material to the patients, nasogastric tube insertion in patients who are unable to tolerate orally administered contrast material, prolonged ED stay and possible delays in diagnosis, treatment, and operative intervention. Prolonged ED stay also results in increased health-care costs and patient discomfort . Many studies have suggested that IV contrast alone is sensitive and specific for the diagnosis of appendicitis . However, insufficient attention has been given in the literature to the impact of oral contrast material on the diagnosis of other bowel-related causes of acute abdominal pain . To the best of our knowledge, no large prospective randomized trial has focused on this influence.
Get Radiology Tree app to read full this article<
Materials and Methods
Patients
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
CT Technique
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Image Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
TABLE 1
The Clinical Characteristics of Our Patients
Study Group ( N = 174) Control Group ( N = 174)P Value Age (mean years ± SD) 48.3 ± 17 48 ± 17.1 0.860 S/P abdominal operation, n (%) 41(23.6) 53(30.5) 0.147 Change in bowel habits, n (%) 18(10.3) 28(16.1) 0.113 Nausea or vomiting, n (%) 35(20.1) 63(36.2) 0.001 Fever(>37.5°C), n (%) 6(3.4) 7(4) 0.777 Neutrophils(mean % ± SD) 69.3 ± 12.6 69.1 ± 12.4 0.876 CRP(median) 7.3 12.7 0.043 Tenderness, n (%) Located 135(77.6) 146(83.9) 0.377 Diffuse 15(8.6) 13(7.5)
CRP, C-reactive protein; S/P, status post; SD, standard deviation.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
TABLE 2
Technical Adequacy of the Studies
Study Group ( N = 174) Control Group ( N = 174)P Value Excellent, n (%) 149(85.6) 157(90.2) 0.134 Good, n (%) 15(8.6) 14(8) Fair, n (%) 10(5.7) 3(1.7)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
TABLE 3
Specific Findings of the Main Bowel-related Pathologies in Both Groups
Study Group Control Group Appendicitis 28 33 Distention Yes/maybe 27 33 No 1 0 Wall thickening Yes 26 32 No 2 1 Wall enhancement Yes/maybe 24 26 No 4 7 Fat stranding Yes/maybe 27 30 No 1 3 Appendicolith Yes 8 7 No 20 26 Collection Yes 3 3 No 25 30 Diverticulitis 17 19 Diverticulosis Yes 17 19 Wall thickening Yes/maybe 17 18 No 0 1 Wall enhancement Yes/maybe 14 16 No 3 3 Fat stranding Yes/maybe 17 19 Specific diverticulum dilatation Yes 8 10 No 9 9 Collection Yes 0 2 No 17 19 Colitis 9 5 Wall thickening Yes/maybe 9 5 Wall enhancement Yes/maybe 6 4 No 3 1 Fat stranding Yes/maybe 8 4 No 1 1 Collection Yes 1 0 No 8 5

Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
TABLE 4
Cases in which Oral Contrast Material Was Considered Useful or Probably Useful
Type of Diagnosis Number of Cases Reason Study group Appendicitis 3 Two cases—low INAF index
One case—unusual location of the appendix between small-bowel loops Enteritis 1 Suspected bowel obstruction Colitis 1 Suspected inflammatory bowel disease No bowel pathology 1 Small-bowel malrotation Control group Appendicitis 2 One case—low INAF index
One case—appendix not filled with OCM Diverticulitis 2 Diverticulum not filled with OCM Colitis 2 OCM filled the entire colon No bowel pathology 1 OCM filled the entire colon Small-bowel obstruction 1 OCM did not fill the bowel distal to the transition point
INAF, intra-abdominal fat; OCM, oral contrast material.
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Johnson P.T., Horton K.M., Mahesh M., et. al.: Multidetector computed tomography for suspected appendicitis: multi-institutional survey of 16-MDCT data acquisition protocols and review of pertinent literature. J Comput Assist Tomogr 2006; 30: pp. 758-764.
2. Rosen M.P., Sands D.Z., Esterbrook Longmaid H., et. al.: Impact of abdominal CT on the management of patients presenting to the emergency department with acute abdominal pain. Am J Roentgenol 2000; 174: pp. 1391-1396.
3. Stoker J., van Randen A., Laméris W., et. al.: Imaging patients with acute abdominal pain (review). Radiology 2009; 253: pp. 31-46.
4. Paulson E.K., Coursey C.A.: CT protocols for acute appendicitis: time for change. Am J Roentgenol 2009; 193: pp. 1268-1271.
5. Anderson S.W., Soto J.A.: Multi-detector row CT of acute non-traumatic abdominal pain: contrast and protocol considerations. Radiol Clin North Am 2012; 50: pp. 137-147.
6. Broder J.S., Hamedani A.G., Liu S.W., et. al.: Emergency department contrast practices for abdominal/pelvic computed tomography-a national survey and comparison with the American College of Radiology Appropriateness Criteria (®). J Emerg Med 2013; 44: pp. 423-433.
7. Huynh L.N., Coughlin B.F., Wolfe J., et. al.: Patient encounter time intervals in the evaluation of emergency department patients requiring abdominopelvic CT: oral contrast versus no contrast. Emerg Radiol 2004; 10: pp. 310-313.
8. Schuur J.D., Chu G., Sucov A.: Effect of oral contrast for abdominal computed tomography on emergency department length of stay. Emerg Radiol 2010; 17: pp. 267-273.
9. Levenson R.B., Camacho M.A., Horn E., et. al.: Eliminating routine oral contrast use for CT in the emergency department: impact on patient throughput and diagnosis. Emerg Radiol 2012; 19: pp. 513-517.
10. Razavi S.A., Johnson J.-O., Kassin M.T., et. al.: The impact of introducing a no oral contrast abdominopelvic CT examination (NOCAPE) pathway on radiology turnaround times, emergency department length of stay, and patient safety. Emerg Radiol 2014; 21: pp. 605-613.
11. Anderson B.A., Salem L., Flum D.R.: Systematic review of whether oral contrast is necessary for the computed tomography diagnosis of appendicitis in adults. Am J Surg 2005; 190: pp. 474-478.
12. Mun S., Ernst R.D., Chen K., et. al.: Rapid CT diagnosis of acute appendicitis with IV contrast material. Emerg Radiol 2006; 12: pp. 99-102.
13. Kepner A.M., Bacasnot J.V., Stahlman B.A.: Intravenous contrast alone vs intravenous and oral contrast computed tomography for the diagnosis of appendicitis in adult ED patient. Am J Emerg Med 2012; 30: pp. 1765-1773.
14. Anderson S.W., Soto J.A., Lucey B.C., et. al.: Abdominal 64-MDCT for suspected appendicitis: the use of oral and IV contrast material versus IV contrast material only. AJR Am J Roentgenol 2009; 193: pp. 1282-1288.
15. Glauser J., Siff J., Emerman C.: Emergency department experience with nonoral contrast computed tomography in the evaluation of patients for appendicitis. J Patient Saf 2014; 10: pp. 154-158.
16. Latifi A., Labruto F., Kaiser S., et. al.: Does enteral contrast increase the accuracy of appendicitis diagnosis?. Radiol Technol 2011; 82: pp. 294-299.
17. Lee S.Y., Coughlin B., Wolfe J.M., et. al.: Prospective comparison of helical CT of the abdomen and pelvis without and with oral contrast in assessing acute abdominal pain in adult emergency department patients. Emerg Radiol 2006; 12: pp. 150-157.
18. Kammerer S., Höink A.J., Wessling J., et. al.: Abdominal and pelvic CT: is positive enteric contrast still necessary? Results of a retrospective observational study. Eur Radiol 2015; 25: pp. 669-678.
19. Uyeda J.W., Yu H., Ramalingam V., et. al.: Evaluation of acute abdominal pain in the emergency setting using computed tomography without oral contrast in patients with body mass index greater than 25. J Comput Assist Tomogr 2015; 39: pp. 681-686.
20. Alabousi A., Patlas M.N., Sne N., et. al.: Is oral contrast necessary for multidetector computed tomography imaging of patients with acute abdominal pain?. Can Assoc Radiol J 2015; 66: pp. 318-322.
21. Laituri C.A., Fraser J.D., Aguayo P., et. al.: The lack of efficacy for oral contrast in the diagnosis of appendicitis by computed tomography. J Surg Res 2011; 170: pp. 100-103.
22. Zangos S., Steenburg S.D., Phillips K.D., et. al.: Acute abdomen: added diagnostic value of coronal reformations with 64-slice multidetector row computed tomography. Acad Radiol 2007; 14: pp. 19-27.
23. Nikolaidis P., Hwang C.M., Miller F.H., et. al.: The nonvisualized appendix: incidence of acute appendicitis when secondary inflammatory changes are absent. AJR Am J Roentgenol 2004; 183: pp. 889-892.
24. Wolfe J.M., Smithline H., Lee S., et. al.: The impact of body mass index on concordance in the interpretation of matched noncontrast and contrast abdominal pelvic computed tomographic scans in ED patients with nontraumatic abdominal pain. Am J Emerg Med 2009; 24: pp. 144-148.
25. Anderson S.W., Rhea J.T., Milch H.N., et. al.: Influence of body habitus and use of oral contrast on reader confidence in patients with suspected acute appendicitis using 64 MDCT. Emerg Radiol 2010; 17: pp. 445-453.