
Rationale and Objectives
Pancreatic lesions are frequently detected in pancreatic phase only, which may lead to false negative findings in CT-guided biopsies. We evaluated the accuracy and complication rate of CT guided biopsies of pancreatic lesions with i.v.-contrast application following needle placement in comparison to biopsy after contrast enhanced CT.
Materials and Methods
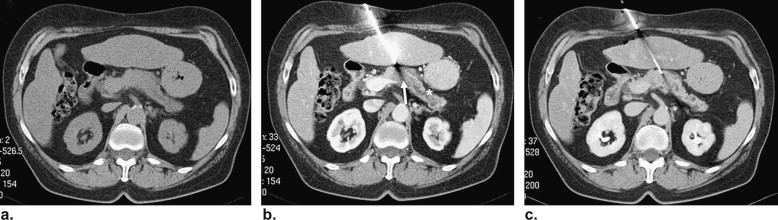
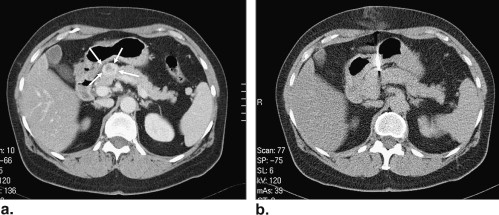
In 30 patients planning and needle placement was performed on the basis of a native planning CT and prior diagnostic CT or MRT. After needle placement contrast enhanced CT was performed to confirm needle course and adjusted if necessary (group 1). In 30 additional patients biopsy was planned based on contrast enhanced CT and needle was placed in the lesion. Control scans confirmed correct needle position (group 2). An 18G coaxial system was used for both groups. Statistical analysis was performed with Student’s t and Fisher’s exact test for comparison of lesion size, location as well as accuracy and complication rates.
Results
Mean lesion size was significantly smaller in group 1 (31 mm vs. 39 mm; p = 0.02). Diagnostic accuracy and sensitivity for malignancy in group 1 was 93% and 92% versus 80% and 77% in group 2. Complications related to the procedure, i.e. haematoma (n = 5, group 1/n = 2, group 2) and pain (n = 0, group 1/n = 2, group 2) did not statistically differ.
Conclusion
CT-guided biopsy of pancreatic lesions with i.v.-contrast application following needle placement is a reliable method and provides superior accuracy compared to biopsies performed after contrast enhanced planning CT.
Computed-tomography (CT)-guided percutaneous biopsy of pancreatic lesions has become commonplace . Biopsies of the pancreas are performed to confirm a diagnosis of malignant pancreatic tumour, mostly ductal adenocarcinoma. Unfortunately, the majority of patients with carcinoma are diagnosed at advanced stage of the disease. Potentially curative resection can be performed in only about 10%–15% of these cases . Without treatment, the median survival time is reported to be only a few months . In several studies, both neoadjuvant radiochemotherapy and palliative chemotherapy were shown to improve survival rates .
However, in addition to the most frequent ductal adenocarcinoma, various other types of tumors with different prognosis and treatment options such as neuroendocrine tumors, lymphomas, ampullary tumors, or acinar carcinomas may give rise to a pancreatic mass. Thus, histologic assessment of any unclear lesion is required to establish the final diagnosis and to exclude patients with pseudotumors or benign lesions which would not undergo aggressive therapies . The sensitivity reported in biopsy studies ranges between 45% and 100% . The low sensitivity in some studies may be explained by the fact that several pancreatic lesions are only detected with cross-sectional imaging in special contrast phase scans, mostly in the arterial/pancreatic phase as hypoattenuating tumors from hypervascularization compared to healthy pancreatic tissue . In CT-guided biopsies, the poor or even absent delineation of the tumor at the time of biopsy/tissue sampling may lead to an increased number of false-negative biopsy findings. Therefore, the aim of our study was to evaluate the accuracy and complication rate of CT-guided biopsies of pancreatic lesions with intravenous contrast application following needle placement in comparison to a contrast-enhanced prebiopsy planning CT.
Material and methods
Patients
Get Radiology Tree app to read full this article<
Table 1
Gender, Mean Age of the Patients, Locations, Mean Sizes of the Lesions in Both Groups
Group 1 Group 2P Value Gender 14 ♂, 16 ♀ 15 ♂, 15 ♀ 1.00 Mean age (y) 63 64 .58 Lesion location (%): .10 Head 80.0 66.7 Body 6.7 26.7 Tail 13.3 6.7 Mean lesion size (mm) All lesions 31 ± 13 ( n = 30) 39 ± 12 ( n = 30) .02 Tumors 32 ± 13 ( n = 25) 39 ± 12 ( n = 27) .05 Nontumors 29 ± 9 ( n = 5) 36 ± 16 ( n = 3) .40 Incorrect diagnoses 27 ± 8 ( n = 2) 39 ± 7 ( n = 6) .10 Malignancy in biopsy_n_ = 23n = 20 0.57 Malignancy in final histology_n_ = 25n = 26 1.00 Correct final diagnosis_n_ = 28n = 24 .25 Complication rates Minor complications 5 4 1.00 Hematomas 5 2 .42 Pain 0 2 .37 Major complications 0 0
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Biopsy Technique
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Standard of Reference and Complications
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Final Diagnoses of the Lesions in Both Groups
Final diagnoses: Group 1 ( n ) Group 2 ( n ) Tumors 25 27 Adenocarcinoma of pancreas 23 26 Carcinoma of choledochus 1 0 Neuroendocrine carcinoma 1 0 Neuroendocrine tumor 0 1 Nontumors 5 3 Chronic pancreatitis 2 2 Cicatricial tissue 0 1 Normal pancreatic tissue 3 0
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Accuracy, Sensitivity and Specificity, Positive Predictive Value, and Negative Predictive Value for Malignancy in Both Groups
Group 1 Group 2 Accuracy 93% 80% Sensitivity 92% 77% Specificity 100% 100% Positive predictive value 100% 100% Negative predictive value 70% 40%
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Complications
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Limitations
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. DelMaschio A., Vanzulli A., Sironi S., et. al.: Pancreatic cancer versus chronic pancreatitis: diagnosis with CA 19-9 assessment, US, CT, and CT-guided fine needle biopsy. Radiology 1991; 178: pp. 95-99.
2. Rodriguez J., Kasberg C., Nipper M., et. al.: CT-guided needle biopsy of the pancreas: a retrospective analysis of diagnostic accuracy. Am J Gastroenterol 1992; 87: pp. 1610-1613.
3. Lüning M., Kursawe R., Schöpke W., et. al.: CT guided percutaneous fine-needle biopsy of the pancreas. Eur J Radiol 1985; 5: pp. 104-108.
4. Brandt K.R., Charboneau J.W., Stephens D.H., et. al.: CT- and US-guided biopsy of the pancreas. Radiology 1993; 187: pp. 99-104.
5. Schima W., Ba-Ssalamah A., Kölblinger C., et. al.: Pancreatic adenocarcinoma. Eur Radiol 2007; 17: pp. 638-649.
6. Boadas J., Balart J., Capella G., et. al.: Survival of cancer of the pancreas. Basis for new strategies in diagnosis and therapy. Rev Esp Enferm Dig 2000; 92: pp. 316-325.
7. Zech C.J., Helmberger T., Wichmann M.W., et. al.: Large core biopsy of the pancreas under CT fluoroscopy control: results and complications. J Comput Assist Tomogr 2002; 26: pp. 743-749.
8. Michl P., Pauls S., Gress T.M.: Evidence-based diagnosis and staging of pancreatic cancer. Best Pract Res Clin Gastroenterol 2006; 20: pp. 227-251.
9. Wittenberg J., Mueller P.R., Ferucci J.T.: Percutaneous core biopsy of abdominal tumors using 22 gauge needles: further observations. AJR Am J Roentgenol 1982; 139: pp. 75-80.
10. Yamada Y., Mori H., Matsumoto S., et. al.: Invasive carcinomas derived from intraductal papillary mucinous neoplasms of the pancreas: a long-term follow-up assessment with CT imaging. J Comput Assist Tomogr 2006; 30: pp. 885-890.
11. McNulty N.J., Francis I.R., Platt J.F., et. al.: Multi-detector row helical CT of the pancreas: effect of contrast-enhanced multiphasic imaging on enhancement of the pancreas, peripancreatic vasculature, and pancreatic adenocarcinoma. Radiology 2001; 220: pp. 97-102.
12. Fletcher J.G., Wiersema M.J., Farrell M.A., et. al.: Pancreatic malignancy: value of arterial, pancreatic, and hepatic phase imaging with multi-detector row CT. Radiology 2003; 229: pp. 81-90.
13. Lu D.S., Vedantham S., Krasny R.M., et. al.: Two-phase helical CT for pancreatic tumors: pancreatic versus hepatic phase enhancement of tumor, pancreas, and vascular structures. Radiology 1996; 199: pp. 697-701.
14. Freeny P.C.: CT diagnosis and staging of pancreatic carcinoma. Eur Radiol 2005; 4: pp. D96-D99.
15. Schueller G., Schima W., Schueller-Weidekamm C., et. al.: Multidetector CT of pancreas: effects of contrast material flow rate and individualized scan delay on enhancement of pancreas and tumor contrast. Radiology 2006; 241: pp. 441-448.
16. Jennings P.E., Donald J.J., Coral A., et. al.: Ultrasound-guided core biopsy. Lancet 1989; 1: pp. 1369-1371.
17. Mueller P.R., Miketic L.M., Simeone J.F., et. al.: Severe acute pancreatitis after percutaneous biopsy of the pancreas. AJR Am J Roentgenol 1988; 151: pp. 493-494.
18. Smith E.H.: Complications of percutaneous abdominal fine-needle biopsy. Radiology 1991; 178: pp. 253-258.
19. Heyer C.M., Reichelt S., Peters S.A., et. al.: Computed tomography-navigated transthoracic core biopsy of pulmonary lesions: which factors affect diagnostic yield and complication rates?. Acad Radiol 2008; 15: pp. 1017-1026.
20. Prokesch R.W., Chow L.C., Beaulieu C.F., et. al.: Isoattenuating pancreatic adenocarcinoma at multi-detector row CT: secondary signs. Radiology 2002; 224: pp. 764-768.
21. Zangos S., Vetter T., Huebner F., et. al.: MR-guided biopsies with a newly designed cordless coil in an open low-field system: initial findings. Eur Radiol 2006; 16: pp. 2044-2050.
22. Karlson B.M., Forsman D.A., Wilander E., et. al.: Efficiency of percutaneous core biopsy in pancreatic tumour diagnosis. Surgery 1996; 120: pp. 75-79.