
Rationale and Objectives
Some deep pelvic abscesses are not accessible through anterior or lateral approaches because of the presence of organs and structures. The objective of this study was to assess the feasibility, safety, tolerability, and efficacy of a percutaneous presacral space approach by reviewing our clinical experience and the literature.
Materials and Methods
The outcomes of 12 patients, who have undergone computed tomography (CT)-guided percutaneous presacral space drainage, were retrospectively reviewed, including demographic, clinical, and morphological data in the medical records.
Results
From August 2010 to June 2015, 98 patients underwent CT-guided percutaneous drainage of pelvis abscesses in our institution. A percutaneous presacral space approach was adopted in 12 cases. The fluid collections were related to postoperative complications in nine patients (75%) and inflammatory or infectious intraabdominal disease in the remaining three patients (acute diverticulitis: n = 1; appendicitis: n = 1; Crohn disease: n = 1) (25%). The mean duration of drainage was 9.5 days (range 3–33). Escherichia coli was the most frequently present microorganism (in 50.0% of the all samples). No procedure-related complications were observed, either during or after the procedure. Drainage was successful in 10 patients (83.3%). Drainage failed in one patient because of massive anastomotic dehiscence. The other one died from pulmonary embolus 10 days after drainage.
Conclusions
When an anterior or lateral transabdominal approach is inaccessible, CT-guided transperineal presacral space approach drainage is a safe, well-tolerated, and effective procedure, except for patients with massive anastomotic dehiscence.
Introduction
As a consequence of postsurgical complications, perforated viscus, or inflammatory bowel disease, deep pelvic abscesses are usually associated with significant morbidity and mortality . Percutaneous drainage (PD) of the lower abdomen and pelvic fluid collections have been reported to contribute to minor invasion with undescended effectiveness compared to a surgical approach . Choice of the most appropriate access route is one of critical factors influencing the outcomes of PD because of the many anatomic obstacles (ie, the pelvic bones, bowel, bladder, iliac vessels, gynecological organs, and nerves) . When an anterior or a lateral approach is not feasible, a computed tomography (CT)-guided approach could provide a useful option.
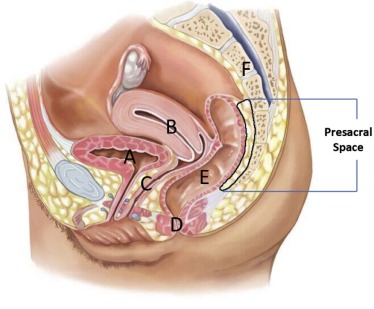
Definition of presacral space is a potential space between the posterior rectal wall and the pelvic surface of the sacrococcyx ( Fig 1 ). Presacral space, bounded anteriorly by the rectal visceral fascia and posteriorly by sacral parietal fascia, is filled with fat, iliac vessels, lymphatics, and other loose connective tissue, but contains no major organs ( Fig 1 ). The expanded presacral space, induced by operation, inflammation, or other reasons, makes it possible to create and dilate an artificial tract between pelvic cavity and skin .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and Methods
Patients and Methods
Get Radiology Tree app to read full this article<
Table 1
Characteristics of the Patients with Pelvic Fluid Abscess Before Drainage
Characteristic Both Conditions ( n = 12) Simple Abscesses ( n = 9) Complex Abscesses ( n = 3)P Value Age, years 53.6(range 17–75) 52.1(range 17–70) 57.6(range 24–75) Sex(male/female), n 7/5 5/4 2/1 .73 Predrainage symptoms \* Fever, n (%) 11(91.7%) 9(100%) 2(66.7%) .25 Abdominal pain, n (%) 9(75.0%) 7(77.8%) 2(66.7%) .7 Distension or abdominal mass, n (%) 5(41.7%) 4(44.4%) 1(33.3%) .74 Tenesmus, n (%) 4(33.3%) 3(33.3%) 1(33.3%) 1 Gastrointestinal hemorrhage, n (%) 1(8.3%) 0(0%) 1(33.3%) .55 Lacunar infarction, n (%) 1(8.3%) 1(11.1%) 0(0%) 1 Etiology Post-colorectal surgery, n (%) 7(58.3%) 6(66.7%) 1(33.3%) .52 Post-peritonitis surgery, n (%) 2(16.7%) 1(11.1%) 1(33.3%) .45 Appendicitis, n (%) 1(8.3%) 1(11.1%) 0(0%) 1 Acute diverticulitis, n (%) 1(8.3%) 1(11.1%) 0(0%) 1 Crohn disease, n (%) 1(8.3%) 0(0%) 1(33.3%) .55 Total, n (%) 12(100%) 9(100%) 3(100%) 1 Distance from tip of coccyx to fluid (mm) † 55 ± 8 55 ± 7 54 ± 10 .85 Largest diameter of pelvic abscess (mm) † 71 ± 24 72 ± 27 67 ± 19 .78 Laboratory data † White blood cell count (×109/L) 15.0 ± 11.4 15.7 ± 13.3 12.7 ± 2.3 .93 C-reactive protein (mg/L) 129.3 ± 104.0 134.1 ± 120.0 115.0 ± 38.6 .8 Erythrocyte sedimentation rate (mm/H) 60.3 ± 34.8 59.0 ± 37.6 64.0 ± 31.1 .84
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Patient Preparation
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Techniques for Drainage
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Post-procedure Catheter Management
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Characteristics of the Patients After Drainage and Follow-up Outcomes
Patients Both Conditions Simple Abscesses( n = 9) Complex Abscesses( n = 3)P Value Pathogen \* Escherichia coli , n (%) 6(50.0%) 4(44.4%) 2(66.7%) 1Pseudomonas aeruginosa , n (%) 4(33.3%) 2(22.2%) 2(66.7%) .236Klebsiella pneumonia , n (%) 5(41.7%) 4(44.4%) 1(33.3%) 1Staphylococcus aureus , n (%) 4(33.3%) 3(33.3%) 1(33.3%) 1Saccharomyces albicans , n (%) 1(8.3%) 1(11.1%) 1(33.3%) .455 Duration of drainage(d) † 9.5 ± 7.8 7.0 ± 2.1 17.0 ± 14.2 .047 Gauge of catheter(F) † 9.7 ± 2.5 9.1 ± 2.3 11.3 ± 3.1 .213 Postdrainage complications † Pulmonary infection, n (%) 2(16.7%) 2(22.2%) 0(0%) 1 Pulmonary embolus, n (%) 1(8.3%) 0(0%) 1(33.3%) .25 Outcomes Complete resolution, n (%) 10(83.3%) 8(88.9%) 2(66.7%) .455 Recurrence of fluid collections, n (%) 1(8.3%) 1(11.1%) 0(0%) 1 Death, n (%) 1(8.3%) 0(0%) 1(33.3%) .25
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Ryan R.S., McGrath F.P., Haslam P.J., et. al.: Ultrasound-guided endocavitary drainage of pelvic abscesses: technique, results and complications. Clin Radiol 2003; 58: pp. 75-79.
2. Golfieri R., Cappelli A.: Computed tomography-guided percutaneous abscess drainage in coloproctology: review of the literature. Tech Coloproctol 2007; 11: pp. 197-208.
3. Duszak R.L., Levy J.M., Akins E.W., et. al.: Percutaneous catheter drainage of infected intra-abdominal fluid collections. American College of Radiology. ACR Appropriateness Criteria. Radiology 2000; 215: pp. 1067-1075.
4. Mirilas P., Skandalakis J.E.: Surgical anatomy of the retroperitoneal spaces part II: the architecture of the retroperitoneal space. Am Surg 2010; 76: pp. 33-42.
5. Harisinghani M.G., Gervais D.A., Hahn P.F., et. al.: CT-guided transgluteal drainage of deep pelvic abscesses: indications, technique, procedure-related complications, and clinical outcome. Radiographics 2002; 22: pp. 1353-1367.
6. Saokar A., Arellano R.S., Gervais D.A., et. al.: Transvaginal drainage of pelvic fluid collections: results, expectations, and experience. AJR Am J Roentgenol 2008; 191: pp. 1352-1358.
7. Harisinghani M.G., Gervais D.A., Maher M.M., et. al.: Transgluteal approach for percutaneous drainage of deep pelvic abscesses: 154 cases. Radiology 2003; 228: pp. 701-705.
8. Sudakoff G.S., Lundeen S.J., Otterson M.F.: Transrectal and transvaginal sonographic intervention of infected pelvic fluid collections: a complete approach. Ultrasound Q 2005; 21: pp. 175-185.
9. Nielsen M.B., Torp-Pedersen S.: Sonographically guided transrectal or transvaginal one-step catheter placement in deep pelvic and perirectal abscesses. AJR Am J Roentgenol 2004; 183: pp. 1035-1036.
10. Siegel R.L., Miller K.D., Jemal A.: Cancer statistics, 2015. CA Cancer J Clin 2015; 65: pp. 5-29.
11. Bang J.Y., Wilcox C.M., Trevino J., et. al.: Factors impacting treatment outcomes in the endoscopic management of walled-off pancreatic necrosis. J Gastroenterol Hepatol 2013; 28: pp. 1725-1732.
12. Varadarajulu S., Drelichman E.R.: EUS-guided drainage of pelvic abscess (with video). Gastrointest Endosc 2007; 66: pp. 372-376.
13. Tasar M., Ugurel M.S., Kocaoglu M., et. al.: Computed tomography-guided percutaneous drainage of splenic abscesses. Clin Imaging 2004; 28: pp. 44-48.
14. Maher M.M., Gervais D.A., Kalra M.K., et. al.: The inaccessible or undrainable abscess: how to drain it. Radiographics 2004; 24: pp. 717-735.
15. Walser E., Raza S., Hernandez A., et. al.: Sonographically guided transgluteal drainage of pelvic abscesses. AJR Am J Roentgenol 2003; 181: pp. 498-500.
16. Gervais D.A., Hahn P.F., O’Neill M.J., et. al.: CT-guided transgluteal drainage of deep pelvic abscesses in children: selective use as an alternative to transrectal drainage. AJR Am J Roentgenol 2000; 175: pp. 1393-1396.
17. Ryan J.M., Murphy B.L., Boland G.W., et. al.: Use of the transgluteal route for percutaneous abscess drainage in acute diverticulitis to facilitate delayed surgical repair. AJR Am J Roentgenol 1998; 170: pp. 1189-1193.
18. Robert B., Chivot C., Fuks D., et. al.: Percutaneous, computed tomography-guided drainage of deep pelvic abscesses via a transgluteal approach: a report on 30 cases and a review of the literature. Abdom Imaging 2013; 38: pp. 285-289.
19. van Doesburg I.A., Boerma D., Bollen T.L., et. al.: Large gluteal abscesses as a complication of transgluteal drainage of pelvic abscesses: analysis of three cases and a search of the literature. Dig Surg 2009; 26: pp. 329-332.