
Rationale and Objectives
The aims of this study were to compare diagnostic accuracy between computed tomography (CT)–guided percutaneous cutting needle biopsy (PCNB) and surgery or open biopsy for thymic epithelial tumors in accordance with the World Health Organization (WHO) classification and to evaluate computed tomographic diagnosis additionally.
Materials and Methods
Subjects were 20 patients (11 men, 9 women) in whom CT, CT-guided PCNB, and surgery had been performed for anterior mediastinal tumors. All diagnoses of both CT-guided PCNB and surgery or open biopsy were made in accordance with the WHO classification. Computed tomographic diagnoses were performed by two radiologists on the basis of radiologic characteristics previously reported according to the simplified WHO classification (types A and AB, type B1, types B2 and B3, and thymic carcinoma). The concordance of the WHO classification or the simplified WHO classification between the diagnosis on either CT or CT-guided PCNB and that on surgery was evaluated using the weighted κ statistic.
Results
The histologic classifications on the basis of surgical resection specimens were as follows: type A, n = 3; type AB, n = 5; type B1, n = 3; type B2, n = 4; type B3, n = 4; and thymic carcinoma, n = 1. The overall concordance with the diagnosis according to the WHO classification established using CT-guided PCNB specimens (weighted κ = 0.757) was higher than that using computed tomographic diagnosis (weighted κ = 0.437).
Conclusion
CT-guided PCNB is a technique with good concordance of the WHO classification of thymic epithelial tumors between the diagnoses of surgery or open biopsy.
In 1999, the World Health Organization (WHO) proposed a consensus classification of thymic epithelial tumors , which was revised in 2004 . It stratifies thymic epithelial tumors into six categories (types A, AB, B1, B2, and B3 and thymic carcinoma) on the basis of epithelial cell morphology and the lymphocyte/epithelial cell ratio. The WHO histologic classification reflects the clinical features of thymic epithelial tumors, and this system may contribute to the clinical assessment and treatment of patients with thymoma . Computed tomography (CT) is commonly used in biopsies to assist with precision guidance of the instruments necessary to perform the biopsies in the appropriate areas of the body. CT-guided biopsy is often preferred because most mediastinal tumors are located adjacent to major vessels and other important structures . Percutaneous cutting needle biopsy (PCNB) has become safer and more accurate by using larger, 18-gauge to 20-gauge needles , which allow sufficient tissue to be obtained for histologic examination and diagnosis of thymic epithelial tumor . However, to our knowledge, only a few studies have assessed the reliability of both CT and CT-guided PCNB for the diagnosis of thymic epithelial tumors according to the WHO classification. The aims of the present study were to compare diagnostic accuracy between CT-guided PCNB and surgery or open biopsy and also to evaluate computed tomographic image diagnosis by radiologists on the basis of previously reported computed tomographic features of thymic epithelial tumors in accordance with the WHO classification.
Materials and Methods
Patients
Subjects were 20 patients (11 men, 9 women; age range, 35–74 years; mean age, 61 years), in whom CT-guided PCNB had been performed for anterior mediastinal tumors between May 2000 and November 2006 and for whom definitive diagnoses of thymic epithelial tumors were established by surgical resection or open surgical biopsy. CT was performed in all patients prior to CT-guided PCNB. Computed tomographic images were obtained before and after contrast medium administration using 8-detector (LightSpeed Ultra; GE Healthcare, Milwaukee, WI; n = 14) and 64-detector (LightSpeed VCT; GE Healthcare; n = 6) computed tomographic scanners. The ethics review boards of the institutions that contributed cases to this study did not require patients’ approval or informed consent for the retrospective review of patient records and images.
CT-guided PCNB
Get Radiology Tree app to read full this article<
Evaluation of the Diagnostic Accuracy of CT-guided PCNB for Thymic Epithelial Tumors
Get Radiology Tree app to read full this article<
Diagnosis According to Computed Tomographic Findings of Thymic Epithelial Tumors
Get Radiology Tree app to read full this article<
Table 1
Referential Diagnostic Criteria on the Basis of Previously Reported Computed Tomographic Features for Thymic Epithelial Tumors in Accordance with the World Health Organization Classification
Probability CT Feature High Low Smooth contour Type A Others Lobulated contour Type B2, type B3, carcinoma Others Calcification Type B1, type B2, type B3 Others Inhomogeneous enhancement Type B2, type B3, carcinoma Others Invasion Type B2, type B3, carcinoma Others Lymphadenopathy Carcinoma Others
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
wij=1−(i−j)2/(I−1), w
i
j
=
1
−
(
i
−
j
)
2
/
(
I
−
1
)
,
where i and j are indices of the categories being used, and I is the number of categories. Interobserver agreement was classified as poor (κ = 0.00–0.20), fair (κ = 0.21–0.40), moderate (κ = 0.41–0.60), good (κ = 0.61–0.80), or excellent (κ = 0.81–1.00).
Get Radiology Tree app to read full this article<
Results
CT-guided PCNB
Get Radiology Tree app to read full this article<
Table 2
Gauges of Cutting Needles and Frequency of Puncture
Needle Gauge Number of Cases Frequency of Puncture CT-guided PCNB Diagnosis Surgical Resection Specimen Diagnosis 14, 16 1 2 AB (1) AB (1) 16 2 2 Carcinoma (1) Carcinoma (1) 3 B1 (1) B1 (1) 18 17 1 A (1) A (1) B3 (1) B3 (1) 2 A (2) A (1) AB (1) AB (3) A (1) AB (2) B1 (7) AB (1) B1 (2) B2 (3) B3 (1) B2 (1) B2 (1) B3 (2) B3 (2)
CT, computed tomography; PCNB, percutaneous cutting needle biopsy.
Values in parentheses are numbers of cases.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Diagnoses of CT, CT-guided PCNB Specimens, and Surgical Resection Specimens
Get Radiology Tree app to read full this article<
Table 3
Computed Tomographic Findings of Thymic Epithelial Tumors in This Study and Diagnoses of CT-guided PCNB Specimens and Surgical Resection Specimens
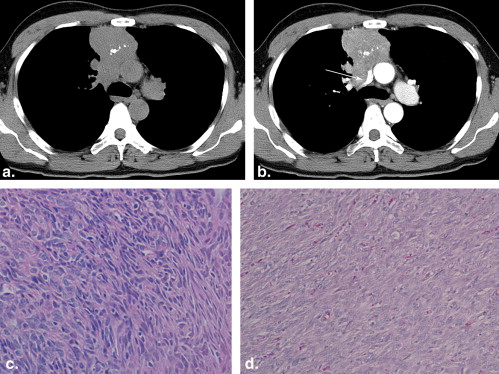
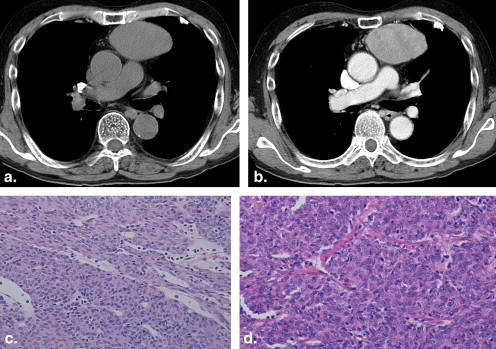
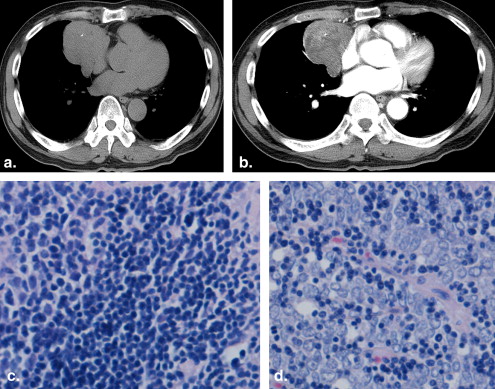
Specimen ∗ Case Size, Long Axis × Short Axis (cm) Contours/Shape LDA Calcification Enhancement LN Invasion Diagnosis by CT CT-guided PCNB Surgical Resection 1 5.0 × 4.8 Lobular/oval − + Inhomogeneous − + 3 1 (A) 1 (A) 2 5.0 × 3.8 Smooth/oval + − Homogeneous − − 1 1 (A) 1 (A) 3 8.0 × 7.2 Smooth/oval + − Homogeneous − − 1 1 (A) 1 (AB) 4 7.0 × 4.7 Lobular/oval − − Homogeneous − − 1 1 (AB) 1 (A) 5 5.1 × 4.5 Lobular/oval + + Inhomogeneous − − 2 1 (AB) 1 (AB) 6 9.0 × 8.2 Lobular/oval + + Inhomogeneous − − 3 1 (AB) 1 (AB) 7 4.8 × 3.3 Lobular/oval − − Homogeneous − − 1 1 (AB) 1 (AB) 8 7.3 × 4.2 Lobular/oval − − Homogeneous − + 3 2 (B1) 3 (B2) 9 5.3 × 3.3 Smooth/oval − − Homogeneous − − 1 2 (B1) 1 (AB) 10 5.0 × 3.6 Lobular/oval − + Homogeneous − + 2 2 (B1) 3 (B2) 11 5.9 × 4.0 Lobular/oval − − Inhomogeneous − − 2 2 (B1) 3 (B2) 12 5.4 × 5.3 Lobular/oval + + Inhomogeneous − + 3 2 (B1) 3 (B3) 13 6.4 × 3.8 Lobular/oval − + Inhomogeneous − + 3 2 (B1) 2 (B1) 14 6.5 × 3.9 Smooth/oval − − Homogeneous − − 1 2 (B1) 2 (B1) 15 7.2 × 3.5 Lobular/oval − + Inhomogeneous − + 3 2 (B1) 2 (B1) 16 5.3 × 3.8 Lobular/oval − − Homogeneous − + 3 3 (B2) 3 (B2) 17 6.7 × 4.7 Smooth/oval − − Inhomogeneous − − 1 3 (B3) 3 (B3) 18 5.7 × 3.5 Lobular/oval + + Inhomogeneous − − 3 3 (B3) 3 (B3) 19 6.2 × 4.1 Lobular/oval + − Inhomogeneous − − 3 3 (B3) 3 (B3) 20 4.2 × 2.6 Lobular/oval + − Inhomogeneous + + 4 4 (carcinoma) 4 (carcinoma)
CT, computed tomography; LDA, low-density area (necrosis or cystic degeneration); LN, lymphadenopathy; PCNB, percutaneous cutting needle biopsy.
Get Radiology Tree app to read full this article<
Table 4
Concordance Between the Diagnoses of CT-guided PCNB Specimen and Those of Surgical Resection Specimens Classified According to the World Health Organization Classification
Diagnosis of the Surgical Resection Specimen CT-guided PCNB Diagnosis A AB B1 B2 B3 Carcinoma Total A 2 1 0 0 0 0 3 AB 1 3 0 0 0 0 4 B1 0 1 3 3 1 0 8 B2 0 0 0 1 0 0 1 B3 0 0 0 0 3 0 3 Carcinoma 0 0 0 0 0 1 1 Total 3 5 3 4 4 1 20
CT, computed tomography; PCNB, percutaneous cutting needle biopsy.
The overall concordance between the diagnosis according to the World Health Organization classification established by PCNB specimen and that by surgical specimen was 65% (weighted κ = 0.757).
Table 5
Concordance Between the Diagnoses of CT and Those of Surgical Resection Specimens Classified According to the Simplified World Health Organization Classification
Diagnosis of the Surgical Resection Specimen Diagnosis on CT A and AB B1 B2 and B3 Carcinoma Total A and AB 5 1 1 0 7 B1 1 0 2 0 3 B2 and B3 2 2 5 0 9 Carcinoma 0 0 0 1 1 Total 8 3 8 1 20
CT, computed tomography.
The overall concordance between the diagnosis according to the World Health Organization classification established by CT and that by the surgical specimen was 55% (weighted κ = 0.437).
Get Radiology Tree app to read full this article<
Cases with Complete Concordance Between Diagnoses of the CT-guided PCNB Specimens and Those of the Surgical Resection Specimens
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Cases with Discrepancies Between Diagnoses of the CT-guided PCNB Specimens and Those of the Surgical Resection Specimen
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Rosai J., Sobin L.H.: Histological typing of tumours of the thymus.International histological classification of tumours.1999.SpringerNew York:
2. Travis W.D.Brambilla E.Muller-Hermelink H.K. et. al.Pathology and genetics: tumors of the lung, pleura, thymus and heart.2004.IARCLyon, France:
3. Okumura M., Ohta M., Tateyama H., et. al.: The World Health Organization histologic classification system reflects the oncological behavior of thymoma: a clinical study of 273 patients. Cancer 2002; 94: pp. 624-632.
4. Chen G., Marx A., Wen-Hu C., et. al.: New WHO histologic classification predicts prognosis of thymic epithelial tumors: a clinicopathologic study of 200 thymoma cases from China. Cancer 2002; 95: pp. 420-429.
5. Chalabreysse L., Roy P., Cordier J.F., et. al.: Correlation of the WHO schema for the classification of thymic epithelial neoplasms with prognosis: a retrospective study of 90 tumors. Am J Surg Pathol 2002; 26: pp. 1605-1611.
6. Kondo K., Yoshizawa K., Tsuyuguchi M., et. al.: WHO histologic classification is a prognostic indicator in thymoma. Ann Thorac Surg 2004; 77: pp. 1183-1188.
7. Klein J.S., Salomon G., Stewart E.A.: Transthoracic needle biopsy with a coaxially placed 20-gauge automated cutting needle: results in 122 patients. Radiology 1996; 198: pp. 715-720.
8. Mueller P.R., vanSonnenberg E.: Interventional radiology in the chest and abdomen. N Engl J Med 1990; 322: pp. 1364-1374.
9. Moulton J.S., Moore P.T.: Coaxial percutaneous biopsy technique with automated biopsy devices: value in improving accuracy and negative predictive value. Radiology 1993; 186: pp. 515-522.
10. Nakagawa K., Asamura H., Matsuno Y., et. al.: Thymoma: a clinicopathologic study based on the new World Health Organization classification. J Thorac Cardiovasc Surg 2003; 126: pp. 1134-1140.
11. Sadohara J., Fujimoto K., Müller N.L., et. al.: Thymic epithelial tumors: comparison of CT and MR imaging findings of low-risk thymomas, high-risk thymomas, and thymic carcinomas. Eur J Radiol 2006; 60: pp. 70-79.
12. Tomiyama N., Johkoh T., Mihara N., et. al.: Using the World Health Organization classification of thymic epithelial neoplasms to describe CT findings. AJR Am J Roentgenol 2002; 179: pp. 881-886.
13. Jeong Y.J., Lee K.S., Kim J., et. al.: Does CT of thymic epithelial tumors enable us to differentiate histologic subtypes and predict prognosis?. AJR Am J Roentgenol 2004; 183: pp. 283-289.
14. Suster S., Rosai J.: Thymic carcinoma: a clinicopathologic study of 60 cases. Cancer 1991; 67: pp. 1025-1032.
15. Giaccone G., Wilmink H., Paul M.A., et. al.: Systemic treatment of malignant thymoma. Am J Clin Oncol 2006; 29: pp. 336-344.
16. Magois E., Guigay J., Blancard P.S., et. al.: Multimodal treatment of thymic carcinoma: report of nine cases. Lung Cancer 2008; 59: pp. 126-132.
17. Rajan A., Giaccone G.: Treatment of advanced thymoma and thymic carcinoma. Curr Treat Options Oncol 2008; 9: pp. 277-287.
18. Herman S.J., Holub R.V., Weisbrod G.L., et. al.: Anterior mediastinal masses: utility of transthoracic needle biopsy. Radiology 1991; 180: pp. 167-170.
19. Weisbrod G.L.: Percutaneous fine-needle aspiration of the mediastinum. Clin Chest Med 1987; 8: pp. 27-41.
20. Protopapas Z., Westcott J.L.: Transthoracic hilar and mediastinal biopsy. J Thorac Imaging 1997; 12: pp. 250-258.
21. Yonemori K., Tsuta K., Tateishi U., et. al.: Diagnostic accuracy of CT-guided percutaneous cutting needle biopsy for thymic tumours. Clin Radiol 2006; 61: pp. 771-775.
22. Suster S.: Primary large-cell lymphomas of the mediastinum. Semin Diag Pathol 1999; 16: pp. 51-64.
23. Pan C.C., Chen P.C., Chiang H.K.I.T.: (CD117) is frequently overexpressed in thymic carcinomas but is absent in thymomas. J Pathol 2004; 202: pp. 375-381.