
Rationale and Objectives
To compare the image quality and diagnostic confidence of low-dose computed tomography (CT) of urololithiasis using filtered back projection (FBP) and iterative reconstruction techniques (IRT).
Materials and Methods
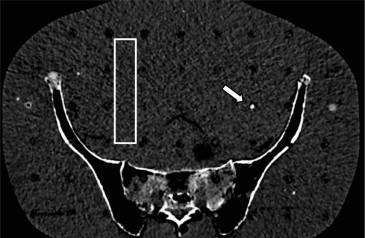
A 4.8 × 4.3 × 5.2 mm 3 uric acid ureteral stone was placed inside an anthropomorphic Alderson phantom at the pelvic level. Fifteen scans were performed on a 64-row dual-source CT system using different tube voltages (80, 100, and 120 kV) and current-time products (8, 15, 30, 70, and 100 mAs). Image reconstruction using FBP and IRT (iterative reconstruction in image space) resulted in 30 data sets. Objective image quality was evaluated by noise measurements. Effective doses were estimated for each data set with use of an established dosimetry program. Subjective image quality and confidence level were rated by two radiologists.
Results
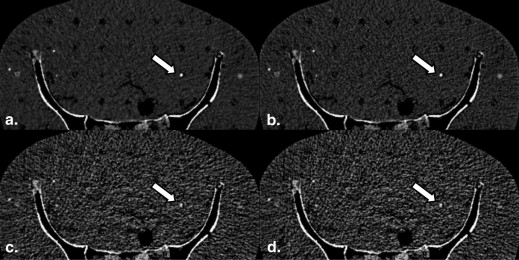
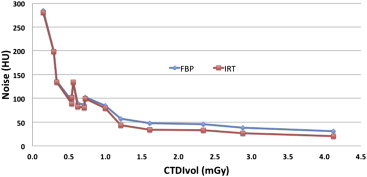
Noise was systematically lower for images reconstructed with IRT compared to FBP (55 ± 30 vs 65 ± 26 Hounsfield units; P = .004) for volume CT dose index values above about 0.6 mGy (or an effective dose of about 0.4 mSv for both sexes). For the 14 scans rated to have diagnostic image quality, the estimated effective doses ranged from 0.3 to 2.5 mSv for males and from 0.4 to 3.1 mSv for females. Subjective image quality and diagnostic confidence for IRT was not significantly better than those for FBP.
Conclusions
In a phantom study for CT of urolithiasis, IRT improves objective image quality compared to FBP above a certain dose threshold. However, this does not translate into improved subjective image quality or a higher degree of confidence for the diagnosis of high-contrast urinary stones.
Nonenhanced multidetector computed tomography (CT) has widely replaced conventional intravenous urography for the examination of patients who present to the emergency department with symptoms of urolithiasis . Nonenhanced CT takes less time than intravenous urography, especially in patients with obstructing calculi, and reduces the patient’s risk for complications due to application of intravenous contrast material. Moreover, nonenhanced CT allows for an effective detection of conditions known to cause unilateral flank pain besides urolithiasis . In addition, CT has been shown to directly impact patient management and guide further care in the emergency department .
However, despite the advantages of CT for the diagnosis of urolithiasis, the inherent radiation exposure applied to young patients presenting with symptoms of urolithiasis continues to raise concerns, particularly for patients undergoing repetitive studies . Along with the increased availability of CT scanners, the number of emergency department visits in the United States associated with a CT scan increased from 2.7 million to 16.2 million annually between 1995 and 2007 according to a study by Larson et al . In their study, symptoms of side or flank pain accounted for 4.6% of all CT-associated visits . Therefore, while measures to reduce ionizing radiation have been successfully implemented in clinical practice, the topic continues to be of interest to both the radiological community and the general public .
Get Radiology Tree app to read full this article<
Materials and methods
Phantom
Get Radiology Tree app to read full this article<
CT System and Protocols
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Data Analysis
Subjective Image Quality
Get Radiology Tree app to read full this article<
Objective Image Quality and Radiation Dose
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Subjective Image Quality and Diagnostic Confidence
Get Radiology Tree app to read full this article<
Table 1
Scan Parameters, Effective Doses, Noise Levels, and Subjective Scores for 30 Computed Tomography Images Reconstructed with the Standard FBP and the Iterative IRIS Algorithm. Scans 1–14 Were Rated to Have Diagnostic Image Quality (bold).
Voltage (kV) Reference Current–Time Product (mAs) Effective Current–Time Product (mAs) Reconstruction Algorithm CTDI vol (mGy) ED, Male (mSv)
(ICRP 103) ED, Female (mSv)
(ICRP 103) Noise
(HU) Image Quality
Reader 1/2 Confidence Level
Reader 1/2112010086FBP4.122.53.1385/53/3212010086IRIS4.122.53.1265/53/331207060FBP2.881.92.2315/53/341207060IRIS2.881.92.2215/53/3510010079FBP2.341.41.8455/53/3610010079IRIS2.341.41.8335/53/371203024FBP1.210.80.9584/43/381007059FBP1.611.01.2484/43/391007059IRIS1.611.01.2344/33/3101203024IRIS1.210.80.9433/33/3111201512FBP0.620.40.5903/32/21212087FBP0.540.40.4953/32/21312087IRIS0.540.40.4893/32/214803030IRIS0.560.30.41343/32/2 15 100 15 13 FBP 0.54 0.3 0.4 105 3/2 2/2 16 100 15 13 IRIS 0.54 0.3 0.4 101 2/3 2/2 17 120 15 12 IRIS 0.62 0.4 0.5 83 2/3 1/2 18 80 100 71 FBP 1 0.6 0.8 85 2/2 2/2 19 80 100 71 IRIS 1 0.6 0.8 78 2/2 2/2 20 80 70 52 FBP 0.72 0.4 0.6 103 2/2 2/2 21 80 70 52 IRIS 0.72 0.4 0.6 100 2/1 2/1 22 100 30 23 FBP 0.71 0.4 0.5 86 1/1 1/1 23 100 30 23 IRIS 0.71 0.4 0.5 80 1/1 1/1 24 80 30 30 FBP 0.56 0.3 0.4 134 1/1 1/1 25 80 15 15 FBP 0.29 0.2 0.2 199 1/1 1/1 26 80 15 15 IRIS 0.29 0.2 0.2 199 1/1 1/1 27 100 8 8 FBP 0.33 0.2 0.3 136 1/1 1/1 28 100 8 8 IRIS 0.33 0.2 0.3 134 1/1 1/1 29 80 8 8 FBP 0.15 0.1 0.1 285 1/1 1/1 30 80 8 8 IRIS 0.15 0.1 0.1 281 1/1 1/1
CTDI vol , volume computed tomography (CT) dose index; ED, effective dose; FBP, filtered back projection; ICRP, International Commission on Radiological Protection; IRIS, iterative reconstruction in image space.
The effective current–time product displayed after the CT scan on the operator’s console that is reduced compared to the nominal value due to automatic exposure control.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Objective Image Quality and Radiation Dose
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Dalrymple N.C., Verga M., Anderson K.R., et. al.: The value of unenhanced helical computerized tomography in the management of acute flank pain. J Urol 1998; 159: pp. 735-740.
2. Abramson S., Walders N., Applegate K.E., et. al.: Impact in the emergency department of unenhanced CT on diagnostic confidence and therapeutic efficacy in patients with suspected renal colic: a prospective survey. 2000 ARRS President’s Award. American Roentgen Ray Society. AJR Am J Roentgenol 2000; 175: pp. 1689-1695.
3. Abujudeh H.H., Kaewlai R., McMahon P.M., et. al.: Abdominopelvic CT increases diagnostic certainty and guides management decisions: a prospective investigation of 584 patients in a large academic medical center. AJR Am J Roentgenol 2011; 196: pp. 238-243.
4. John B.S., Patel U., Anson K.: What radiation exposure can a patient expect during a single stone episode?. J Endourol 2008; 22: pp. 419-422.
5. Brenner D.J., Hall E.J.: Computed tomography–an increasing source of radiation exposure. N Engl J Med 2007; 357: pp. 2277-2284.
6. Larson D.B., Johnson L.W., Schnell B.M., et. al.: National trends in CT use in the emergency department: 1995-2007. Radiology 2011; 258: pp. 164-173.
7. Amis E.S., Butler P.F.: ACR white paper on radiation dose in medicine: three years later. J Am Coll Radiol 2010; 7: pp. 865-870.
8. May M.S., Wust W., Brand M., et. al.: Dose reduction in abdominal computed tomography: intraindividual comparison of image quality of full-dose standard and half-dose iterative reconstructions with dual-source computed tomography. Invest Radiol 2011; 46: pp. 465-470.
9. Prakash P., Kalra M.K., Kambadakone A.K., et. al.: Reducing abdominal CT radiation dose with adaptive statistical iterative reconstruction technique. Invest Radiol 2010; 45: pp. 202-210.
10. Kulkarni N.M., Uppot R.N., Eisner B.H., et. al.: Radiation dose reduction at multidetector CT with adaptive statistical iterative reconstruction for evaluation of urolithiasis: how low can we go?. Radiology 2012; 265: pp. 158-166.
11. Schabel C., Fenchel M., Schmidt B., et. al.: Clinical evaluation and potential radiation dose reduction of the novel sinogram-affirmed iterative reconstruction technique (SAFIRE) in abdominal computed tomography angiography. Acad Radiol 2012;
12. Yanagawa M., Honda O., Yoshida S., et. al.: Adaptive statistical iterative reconstruction technique for pulmonary CT: image quality of the cadaveric lung on standard- and reduced-dose CT. Acad Radiol 2010; 17: pp. 1259-1266.
13. Becker H.C., Augart D., Karpitschka M., et. al.: Radiation exposure and image quality of normal computed tomography brain images acquired with automated and organ-based tube current modulation multiband filtering and iterative reconstruction. Invest Radiol 2012; 47: pp. 202-207.
14. The 2007 Recommendations of the International Commission on Radiological Protection. ICRP publication 103. Ann ICRP 2007; 37: pp. 1-332.
15. Smith-Bindman R., Lipson J., Marcus R., et. al.: Radiation dose associated with common computed tomography examinations and the associated lifetime attributable risk of cancer. Arch Intern Med 2009; 169: pp. 2078-2086.
16. Fahmy N.M., Elkoushy M.A., Andonian S.: Effective radiation exposure in evaluation and follow-up of patients with urolithiasis. Urology 2012; 79: pp. 43-47.
17. Ferrandino M.N., Bagrodia A., Pierre S.A., et. al.: Radiation exposure in the acute and short-term management of urolithiasis at 2 academic centers. J Urol 2009; 181: pp. 668-672. discussion 73
18. Renker M., Nance J.W., Schoepf U.J., et. al.: Evaluation of heavily calcified vessels with coronary CT angiography: comparison of iterative and filtered back projection image reconstruction. Radiology 2011; 260: pp. 390-399.
19. Funama Y., Oda S., Utsunomiya D., et. al.: Coronary artery stent evaluation by combining iterative reconstruction and high-resolution kernel at coronary CT angiography. Acad Radiol 2012; 19: pp. 1324-1331.
20. Preminger G.M., Tiselius H.G., Assimos D.G., et. al.: 2007 Guideline for the management of ureteral calculi. Eur Urol 2007; 52: pp. 1610-1631.
21. Stolzmann P., Leschka S., Scheffel H., et. al.: Characterization of urinary stones with dual-energy CT: improved differentiation using a tin filter. Invest Radiol 2010; 45: pp. 1-6.
22. Thomas C., Krauss B., Ketelsen D., et. al.: Differentiation of urinary calculi with dual energy CT: effect of spectral shaping by high energy tin filtration. Invest Radiol 2010; 45: pp. 393-398.