
Rationale and Objectives
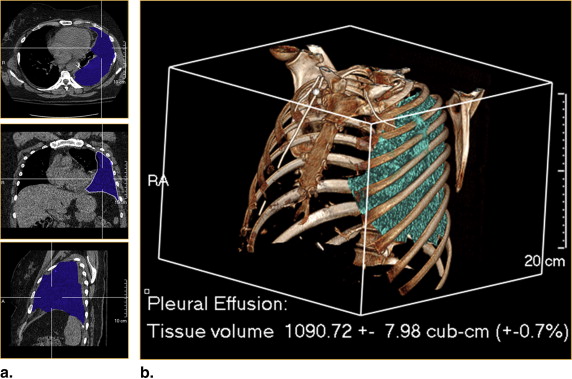
The primary objective of this study was to compare computed tomography (CT) volumetric analysis of pleural effusions with thoracentesis volumes. The secondary objective of this study was to compare subjective grading of pleural effusion size with thoracentesis volumes.
Materials and Methods
This was a retrospective study of 67 patients with free-flowing pleural effusions who underwent therapeutic thoracentesis. CT volumetric analysis was performed on all patients; the CT volumes were compared with the thoracentesis volumes. In addition, the subjective grading of pleural effusion size was compared with the thoracentesis volumes.
Results
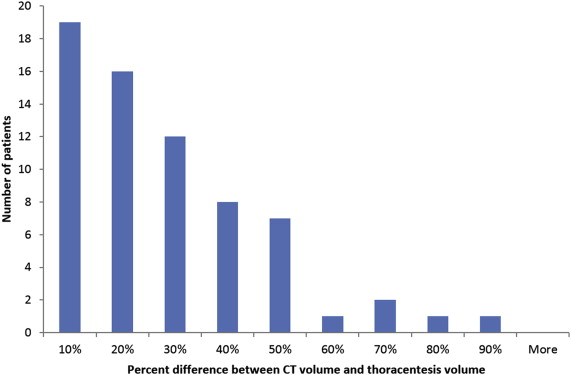
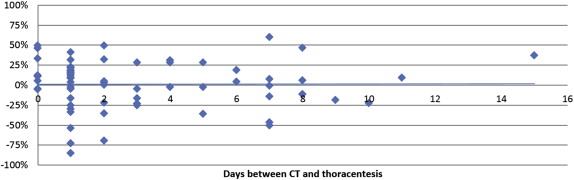
The average difference between CT volume and thoracentesis volume was 9.4 mL (1.3%) ± 290 mL (30%); these volumes were not statistically different ( P = .79, paired two-tailed Student’s t -test). The thoracentesis volume of a “small,” “moderate,” and “large” pleural effusion, as graded on chest CT, was found to be approximately 410 ± 260 cc, 770 ± 270 mL and 1370 ± 650 mL, respectively; the thoracentesis volume of a “small,” “moderate,” and “large” pleural effusion, as graded on chest radiograph, was found to be approximately 610 ± 320 mL, 1040 ± 460 mL, and 1530 ± 830 mL, respectively.
Conclusions
CT volumetric analysis is an accessible tool that can be used to accurately quantify the size of pleural effusions.
A pleural effusion is a pathologic accumulation of fluid in the pleural space. It is a common finding, which can occur in response to a variety of insults, including infection, malignancy, pulmonary embolism, connective tissue disease, congestive heart failure, cirrhosis, and trauma . Although the presence of a pleural effusion is nonspecific, associated findings such as cardiomegaly, consolidation, and lung masses often suggest its etiology .
Pleural effusions can be diagnosed by routine chest radiography, ultrasonography, computed tomography, and magnetic resonance imaging . Even in cases where pleural effusions are diagnosed on physical examination alone, imaging is often warranted to further characterize the pleural effusion and/or estimate its size. Although ultrasound is well-suited for characterizing pleural effusions, computed tomography (CT) is superior in evaluating the size of pleural effusions . In addition, CT can be used to determine the attenuation of a pleural effusion and to visualize reactive pleural thickening or enhancement, which can provide clues to the nature of a pleural effusion .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Get Radiology Tree app to read full this article<
Table 1
Subject Enrollment: Inclusion and Exclusion Criteria

CT, computed tomography.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Pitfalls in Pleural Effusion Tracing
Pitfall Effect Comments Accidental inclusion of adjacent soft tissue Most commonly occurs with collapsed lung and mediastinal structures. Results in overestimation of pleural effusion. IV contrast helps differentiate fluid from adjacent soft tissue. Multiplanar reformats can also help in defining the anatomy. Tracing in a nonoptimal plane Tracing in a nonoptimal plane can be challenging and is often prone to error. The optimal plane is the plane where the pleural effusion can be smoothly traced without discontinuity. Motion and beam hardening artifacts Artifacts can obscure pleural fluid boundaries. Motion artifact is frequently worst near the diaphragms, whereas beam hardening is frequently worst near the apices. Minimize artifacts with optimal CT scanning technique. Complex or loculated pleural effusions Complex pleural effusions can be tedious and time-consuming to trace. More prone to tracing error. May require multiple traces to fully analyze a multicomponent pleural effusion.
CT, computed tomography; IV, intravenous.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Henschke C.I., Davis S.D., Romano P.M., et. al.: Pleural effusions: pathogenesis, radiologic evaluation, and therapy. J Thorac Imaging 1989; 4: pp. 49-60.
2. Jimenez D., Diaz G., Gil D., et. al.: Etiology and prognostic significance of massive pleural effusions. Respir Med 2005; 99: pp. 1183-1187.
3. Light R.W.: A new classification of parapneumonic effusions and empyema. Chest 1995; 108: pp. 299-301.
4. Evans A.L., Gleeson F.V.: Radiology in pleural disease: state of the art. Respirology 2004; 9: pp. 300-312.
5. Light R.W.: Clinical practice. Pleural effusion. N Engl J Med 2002; 346: pp. 1971-1977.
6. Hooper C., Lee Y.C., Maskell N., BTS Pleural Guideline Group: Investigation of a unilateral pleural effusion in adults: British Thoracic Society Pleural Disease Guideline 2010. Thorax 2010; 65: pp. ii4-17.
7. Eibenberger K.L., Dock W.I., Ammann M.E., et. al.: Quantification of pleural effusions: sonography versus radiography. Radiology 1994; 191: pp. 681-684.
8. Kitazono M.T., Lau C.T., Parada A.N., et. al.: Differentiation of pleural effusions from parenchymal opacities: accuracy of bedside chest radiography. AJR Am J Roentgenol 2010; 194: pp. 407-412.
9. Cartaxo A.M., Vargas F.S., Salge J.M., et. al.: Improvements in the 6-min walk test and spirometry following thoracentesis for symptomatic pleural effusions. Chest 2011; 139: pp. 1424-1429.
10. Estenne M., Yernault J.C., De Troyer A.: Mechanism of relief of dyspnea after thoracocentesis in patients with large pleural effusions. Am J Med 1983; 74: pp. 813-819.
11. Klecka M.E., Maldonado F.: Symptom relief after large-volume thoracentesis in the absence of lung perfusion. Chest 2014; 145: pp. 1141-1143.
12. Marcondes B.F., Vargas F., Paschoal F.H., et. al.: Sleep in patients with large pleural effusion: impact of thoracentesis. Sleep Breath 2012; 16: pp. 483-489.
13. Talmor M., Hydo L., Gershenwald J.G., et. al.: Beneficial effects of chest tube drainage of pleural effusion in acute respiratory failure refractory to positive end-expiratory pressure ventilation. Surgery 1998; 123: pp. 137-143.
14. Goligher E.C., Leis J.A., Fowler R.A., et. al.: Utility and safety of draining pleural effusions in mechanically ventilated patients: a systematic review and meta-analysis. Crit Care 2011; 15: pp. R46.
15. Razazi K., Thille A.W., Carteaux G., et. al.: Effects of pleural effusion drainage on oxygenation, respiratory mechanics, and hemodynamics in mechanically ventilated patients. Ann Am Thorac Soc 2014; 11: pp. 1018-1024.
16. Blackmore C.C., Black W.C., Dallas R.V., et. al.: Pleural fluid volume estimation: a chest radiograph prediction rule. Acad Radiol 1996; 3: pp. 103-109.
17. Woodring J.H.: Recognition of pleural effusion on supine radiographs: how much fluid is required?. AJR Am J Roentgenol 1984; 142: pp. 59-64.
18. Mergo P.J., Helmberger T., Didovic J., et. al.: New formula for quantification of pleural effusions from computed tomography. J Thorac Imaging 1999; 14: pp. 122-125.
19. Mironov O., Ishill N.M., Mironov S., et. al.: Pleural effusion detected at CT prior to primary cytoreduction for stage III or IV ovarian carcinoma: effect on survival. Radiology 2011; 258: pp. 776-784.
20. Moy M.P., Levsky J.M., Berko N.S., et. al.: A new, simple method for estimating pleural effusion size on CT scans. Chest 2013; 143: pp. 1054-1059.
21. Brown N.E., Zamel N., Aberman A.: Changes in pulmonary mechanics and gas exchange following thoracocentesis. Chest 1978; 74: pp. 540-542.
22. Wang J.S., Tseng C.H.: Changes in pulmonary mechanics and gas exchange after thoracentesis on patients with inversion of a hemidiaphragm secondary to large pleural effusion. Chest 1995; 107: pp. 1610-1614.
23. Light R.W., Stansbury D.W., Brown S.E.: The relationship between pleural pressures and changes in pulmonary function after therapeutic thoracentesis. Am Rev Respir Dis 1986; 133: pp. 658-661.
24. Perpina M., Benlloch E., Marco V., et. al.: Effect of thoracentesis on pulmonary gas exchange. Thorax 1983; 38: pp. 747-750.
25. Ahmed S.H., Ouzounian S.P., Dirusso S., et. al.: Hemodynamic and pulmonary changes after drainage of significant pleural effusions in critically ill, mechanically ventilated surgical patients. J Trauma 2004; 57: pp. 1184-1188.
26. Walden A.P., Garrard C.S., Salmon J.: Sustained effects of thoracocentesis on oxygenation in mechanically ventilated patients. Respirology 2010; 15: pp. 986-992.
27. Anderson S.A., Danelson K.A., Mammarappallil J.G., et. al.: Semiautomatic method of quantifying pleural effusions using computed tomography scans - Biomed 2013. Biomed Sci Instrum 2013; 49: pp. 13-19.
28. Yao J., Han W., Summers R.M.: Computer aided evaluation of pleural effusion using chest CT images. Proc IEEE Int Symp Biomed Imaging 2009; 2009: pp. 241-244.