
Rationale and Objectives
The aim of this study was to apply a decision analytic model for the evaluation of coronary artery disease (CAD) to define the optimal utilization of coronary computed tomographic angiography (cCTA) and stress testing.
Materials and Methods
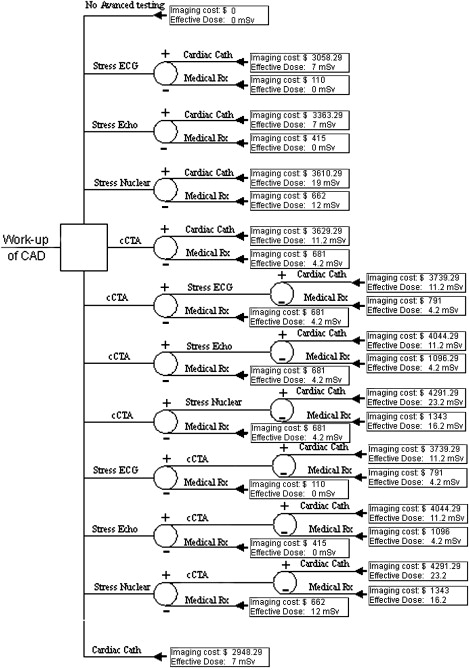
The model tested in this study assumes that CAD is evaluated with a stress test and/or cCTA and that a patient with positive evaluation results undergoes cardiac catheterization. On the basis of values of sensitivity, specificity, and radiation dose from the published literature and test costs from the Medicare fee schedule, a decision tree model was constructed as a function of disease prevalence.
Results
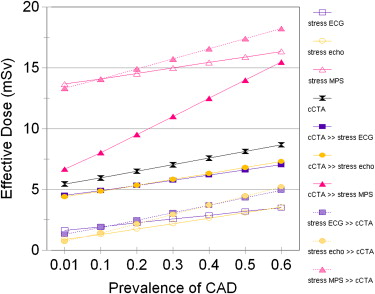
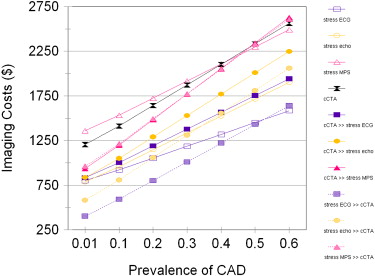
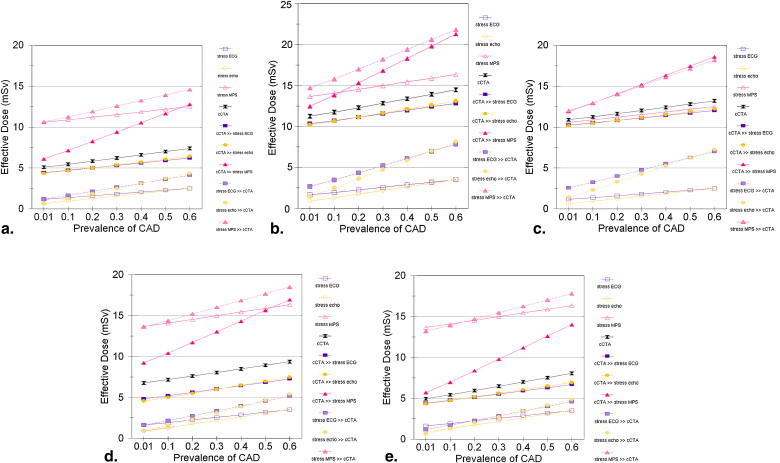
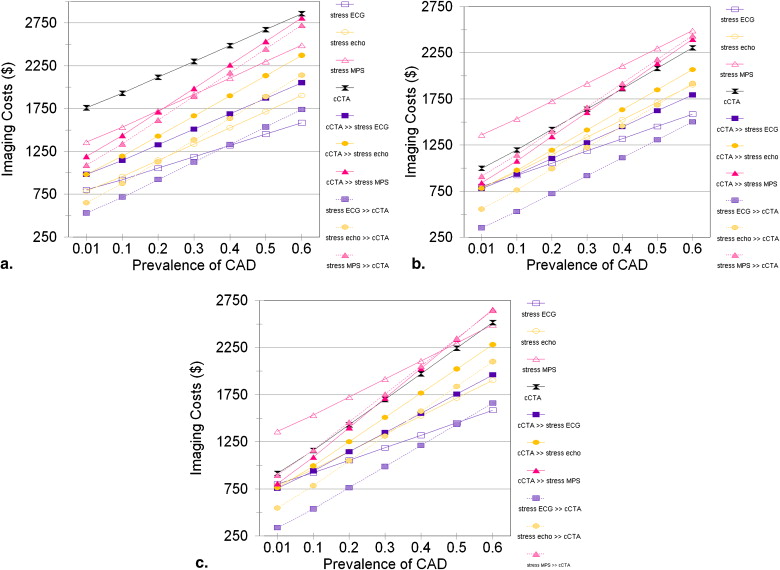
The false-negative rate is lowest when cCTA is used as an isolated test. The false-positive rate is minimized when cCTA is used in combination with stress echocardiography. Effective radiation is minimized by use of stress electrocardiography or stress echocardiography alone or prior to cCTA. When the pretest probability of CAD is low, a strategy that uses stress echocardiography followed by cCTA minimizes the false-positive rate and effective radiation exposure, with relatively low imaging costs and with a false-negative rate only slightly higher than a strategy including stress myocardial scintigraphy. As the pretest probability of CAD increases above 20%, the false-negative rate of stress echocardiography followed by cCTA increases by >5% relative to cCTA alone.
Conclusion
Effective radiation dose and imaging costs for the workup of CAD may be minimized by an appropriate combination of stress testing and cCTA. A strategy that uses stress echocardiography followed by cCTA is most appropriate for the evaluation of low-risk patients with CAD with a pretest probability < 20%, while cCTA alone may be more appropriate in intermediate-risk patients.
Although the age-adjusted death rate from heart disease has been declining slowly over the past 50 years, heart disease remains the most common cause of death in the United States and was responsible for 26% of all deaths in 2006 . Atherosclerotic disease of the coronary arteries remains the most important etiology of heart disease. The evaluation of suspected coronary artery disease (CAD) should always begin with an appropriate history, physical examination, and electrocardiography (ECG). In stable, symptomatic patients, evaluation for CAD often progresses to noninvasive stress testing. Stress testing provides a physiologic evaluation of cardiac function and serves as a diagnostic study and prognostic marker for future coronary events .
Coronary computed tomographic angiography (cCTA) provides a noninvasive alternative to cardiac catheterization for the visualization of coronary anatomy and has demonstrated high sensitivity and specificity for the anatomic presence of CAD . Although functional information about wall motion can be obtained during cCTA, the primary utility of cCTA is for imaging the coronary arteries to define the presence of CAD. Stress testing provides additional information to predict the functional relevance of coronary stenosis with respect to myocardial ischemia . When cCTA demonstrates coronary stenosis of uncertain hemodynamic significance, a follow-up stress test may evaluate the functional significance of CAD found by cCTA. Given the divergent emphases of stress testing on functional physiology and cCTA on coronary anatomy, these two modalities may provide complementary information in the evaluation of CAD .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Sensitivity and Specificity Values Used for Decision Analysis
Modality Sensitivity (by Patient) Specificity (by Patient) Stress ECG 0.68 0.77 Stress echocardiography 0.76 0.88 Stress MPS 0.88 0.77 cCTA Base model: Budoff et al 0.95 0.83 Low specificity: Meijboom et al 0.99 0.64 High specificity: Miller et al 0.85 0.90 Meta-analysis: Vanhoenacker et al 0.99 0.93
cCTA, coronary computed tomographic angiography; ECG, electro-cardiography; MPS, myocardial perfusion scintigraphy.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Effective Radiation Dose
Reference Effective Radiation Dose (mSv) Stress MPS 9.4–12.0 cCTA 4.2–10.0 Cardiac catheterization 5–7
cCTA, coronary computed tomographic angiography; MPS, myo-cardial perfusion scintigraphy.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Diagnostic Testing and Imaging Costs
Diagnostic Test_CPT_ Codes Medicare Fee Schedule Stress ECG 93015 $110 Stress echocardiography 93015, 93351 $415 Stress MPS 78465, 78478, 78480 $662 cCTA 0146T, 0151T $681 Cardiac catheterization Physician fee 93510, 93543, 93556, 93545 $354.29 Facility fee National average facility fee $2594 Total Physician fee + facility fee $2948.29
cCTA, coronary computed tomographic angiography; CPT , Current Procedural Terminology ; ECG, electrocardiography; MPS, myocar-dial perfusion scintigraphy.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
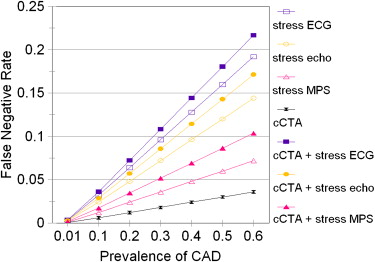
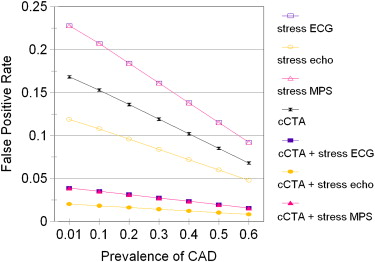
Table 4
Positive and Negative Testing Rates as a Function of Disease Prevalence
Workup Strategy CAD Prevalence (%) TPR (%) TNR (%) FPR (%) FNR (%) Stress ECG 1 0.68 76 23 0.32 Stress echocardiography 1 0.76 87 12 0.24 Stress nuclear 1 0.88 76 23 0.12 cCTA 1 0.95 82 17 0.05 cCTA » stress ECG 1 0.65 95 3.9 0.35 cCTA » stress echocardiography 1 0.72 97 2.0 0.28 cCTA » stress nuclear 1 0.84 95 3.9 0.16 Stress ECG » cCTA 1 0.65 95 3.9 0.35 Stress echocardiography » cCTA 1 0.72 97 2.0 0.28 Stress nuclear » cCTA 1 0.84 95 3.9 0.16 Stress ECG 20 13.6 61.6 18.4 6.4 Stress echocardiography 20 15.2 70.4 9.6 4.8 Stress nuclear 20 17.6 61.6 18.4 2.4 cCTA 20 19.0 66.4 13.6 1 cCTA » stress ECG 20 12.9 76.9 3.1 7.1 cCTA » stress echocardiography 20 14.4 78.4 1.6 5.6 cCTA » stress nuclear 20 16.7 76.9 3.1 3.3 Stress ECG » cCTA 20 12.9 76.9 3.1 7.1 Stress echocardiography » cCTA 20 14.4 78.4 1.6 5.6 Stress nuclear » cCTA 20 16.7 76.9 3.1 3.3 Stress ECG 50 34 38.5 11.5 16 Stress echocardiography 50 38 44.0 6.0 12 Stress nuclear 50 44 38.5 11.5 6 cCTA 50 47.5 41.5 8.5 2.5 cCTA » stress ECG 50 32.3 48.0 2.0 17.7 cCTA » stress echocardiography 50 36.1 49.0 1.0 13.9 cCTA » stress nuclear 50 41.8 48.0 2.0 8.2 Stress ECG » cCTA 50 32.3 48.0 2.0 17.7 Stress echocardiography » cCTA 50 36.1 49.0 1.0 13.9 Stress nuclear » cCTA 50 41.8 48.0 2.0 8.2
CAD, Coronary artery disease; cCTA, coronary computed tomographic angiography; ECG, electrocardiography; FNR, false-negative rate; FPR, false-positive rate; MPS, myocardial perfusion scintigraphy; TNR, true-negative rate; TPR, true-positive rate.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Heron M., Hoyert D.L., Murphy S.L., Xu J., Kochanek K.D., Tejada-Vera B.: Deaths: final data for 2006. Natl Vital Stat Rep 2009; 57: pp. 1-135. Available at: http://www.cdc.gov/nchs/data/nvsr/nvsr57/nvsr57_14.pdf . Accessed January 20, 2010
2. Lee T.H., Boucher C.A.: Noninvasive tests in patients with stable coronary artery disease. N Engl J Med 2001; 344: pp. 1840-1845.
3. Vanhoenacker P.K., Heijenbrok-Kal M.H., Van Heste R., et. al.: Diagnostic performance of multidetector CT angiography for assessment of coronary artery disease: meta-analysis. Radiology 2007; 244: pp. 419-428.
4. Meijer A.B., O Yl , Geleijns J., Kroft L.J.: Meta-analysis of 40- and 64-MDCT angiography for assessing coronary artery stenosis. AJR Am J Roentgenol 2008; 191: pp. 1667-1675.
5. Hacker M., Jakobs T., Hack N., et. al.: Sixty-four slice spiral CT angiography does not predict the functional relevance of coronary artery stenoses in patients with stable angina. Eur J Nucl Med Mol Imaging 2007; 34: pp. 4-10.
6. Gaemperli O., Schepis T., Valenta I., et. al.: Functionally relevant coronary artery disease: comparison of 64-section CT angiography with myocardial perfusion SPECT. Radiology 2008; 248: pp. 414-423.
7. Schuijf J.D., Bax J.J.: CT angiography: an alternative to nuclear perfusion imaging?. Heart 2008; 94: pp. 255-257.
8. Budoff M.J., Rasouli M.L., Shavelle D.M., et. al.: Cardiac CT angiography (CTA) and nuclear myocardial perfusion imaging (MPI)—a comparison in detecting significant coronary artery disease. Acad Radiol 2007; 14: pp. 252-257.
9. Hendel R.C., Patel M.R., Kramer C.M., et. al., American College of Cardiology Foundation Quality Strategic Directions Committee Appropriateness Criteria Working Group; American College of Radiology; Society of Cardiovascular Computed Tomography; Society for Cardiovascular Magnetic Resonance; American Society of Nuclear Cardiology; North American Society for Cardiac Imaging; Society for Cardiovascular Angiography and Interventions; Society of Interventional Radiology: ACCF/ACR/SCCT/SCMR/ASNC/NASCI/SCAI/SIR 2006 appropriateness criteria for cardiac computed tomography and cardiac magnetic resonance imaging: a report of the American College of Cardiology Foundation Quality Strategic Directions Committee Appropriateness Criteria Working Group, American College of Radiology, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, American Society of Nuclear Cardiology, North American Society for Cardiac Imaging, Society for Cardiovascular Angiography and Interventions, and Society of Interventional Radiology. J Am Coll Cardiol 2006; 48: pp. 1475-1497.
10. Gianrossi R., Detrano R., Mulvihill D., et. al.: Exercise-induced ST depression in the diagnosis of coronary artery disease. A meta-analysis. Circulation 1989; 80: pp. 87-98.
11. Garger A.M., Solomon N.A.: Cost-effectiveness of alternative test strategies for the diagnosis of coronary artery disease. Ann Intern Med 1999; 130: pp. 719-728.
12. Budoff M.J., Dowe D., Jollis J.G., et. al.: Diagnostic performance of 64-multidetector row coronary computed tomographic angiography for evaluation of coronary artery stenosis in individuals without known coronary artery disease: results from the prospective multicenter ACCURACY (Assessment by Coronary Computed Tomographic Angiography of Individuals Undergoing Invasive Coronary Angiography) trial. J Am Coll Cardiol 2008; 52: pp. 1724-1732.
13. Meijboom W.B., Meijs M.F., Schuijf J.D., et. al.: Diagnostic accuracy of 64-slice computed tomography coronary angiography. J Am Coll Cardiol 2008; 52: pp. 2135-2144.
14. Miller J.M., Rochitte C.E., Dewey M., et. al.: Diagnostic performance of coronary angiography by 64-row CT. N Engl J Med 2008; 359: pp. 2324-2336.
15. Valentin J., Valentin D.J.: Radiation dose to patients from radiopharmaceuticals: (addendum 2 to ICRP publication 53) approved by the commission in September 1997. Ann ICRP 1998; 28: pp. 1-123.
16. Mettler F.A., Huda W., Yoshizumi T.T., Mahesh M.: Effective doses in radiology and diagnostic nuclear medicine: a catalog. Radiology 2008; 248: pp. 254-263.
17. Hirai N., Horiguchi J., Fujioka C., et. al.: Prospective versus retrospective ECG-gated 64-detector coronary CT angiography: assessment of image quality, stenosis, and radiation dose. Radiology 2008; 248: pp. 424-430.
18. Shuman W.P., Branch K.R., May J.M., et. al.: Prospective versus retrospective ECG gating for 64-detector CT of the coronary arteries: comparison of image quality and patient radiation dose. Radiology 2008; 248: pp. 431-437.
19. Raff G.L., Chinnaiyan K.M., Share D.A., et. al.: Advanced Cardiovascular Imaging Consortium Co-Investigators. Radiation dose from cardiac computed tomography before and after implementation of radiation dose-reduction techniques. JAMA 2009; 301: pp. 2340-2348.
20. Coles D.R., Smail M.A., Negus I.S., et. al.: Comparison of radiation doses from multislice computed tomography coronary angiography and conventional diagnostic angiography. J Am Coll Cardiol 2006; 47: pp. 1840-1845.
21. Gerber T.C., Carr J.J., Arai A.E., et. al.: Ionizing radiation in cardiac imaging: a science advisory from the American Heart Association Committee on Cardiac Imaging of the Council on Clinical Cardiology and Committee on Cardiovascular Imaging and Intervention of the Council on Cardiovascular Radiology and Intervention. Circulation 2009; 119: pp. 1056-1065.
22. Boston Scientific Corporation. Reimbursement. Available at: http://www.bostonscientific.com/Reimbursement . Accessed January 20, 2010.
23. Diamond G.A., Forrester J.S.: Analysis of probability as an aid in the clinical diagnosis of coronary-artery disease. N Engl J Med 1979; 300: pp. 1350-1358.
24. Heijenbrok-Kal M.H., Fleischmann K.E., Hunink M.G.: Stress echocardiography, stress single-photon-emission computed tomography and electron beam computed tomography for the assessment of coronary artery disease: a meta-analysis of diagnostic performance. Am Heart J 2007; 154: pp. 415-423.
25. Boden W.E., O’Rourke R.A., Teo K.K., et. al., COURAGE Trial Research Group: Optimal medical therapy with or without PCI for stable coronary disease. N Engl J Med 2007; 356: pp. 1503-1516.
26. Shaw L.J., Berman D.S., Maron D.J., et. al.: COURAGE Investigators. Optimal medical therapy with or without percutaneous coronary intervention to reduce ischemic burden: Results from the Clinical Outcomes Utilizing Revascularization and Aggressive Drug Evaluation (COURAGE) trial nuclear substudy. Circulation 2008; 117: pp. 1283-1291.
27. Weintraub W.S., Spertus J.A., Kolm P., et. al., COURAGE Trial Research Group: Effect of PCI on quality of life in patients with stable coronary disease. N Engl J Med 2008; 359: pp. 677-687.