
Health outcomes research is essential to align radiology with current standards of high-value patient care, through the assessment of end results of diagnostic tests, interventions, or policy on patient health. To bridge studies of diagnostic test accuracy and health outcomes research, key considerations include: (1) how to determine when a diagnostic test merits evaluation of impact on outcomes, (2) when study of intermediate/surrogate outcomes can be useful, (3) how to consider the possible harms as well as potential benefits of a test, and (4) how to integrate evidence of an imaging test’s efficacy/effectiveness with clinical data to assess outcomes. Due to challenges in conducting studies of long-term outcomes consequent to imaging use, intermediate health outcomes may capture a test’s impact on successful diagnosis and therapy, and can provide readily measurable, incremental insights into the role of imaging in health-care delivery and efficiency. In an era marked by recognition of quality and value of care, outcomes research will provide essential evidence to inform radiologists’ guidance of imaging use toward improved patient care, creation of clinical guidelines, and policy decisions.
Introduction
The development and dissemination of new and improved diagnostic imaging tests have thrived over the past several decades. Disease detection and characterization for medical decision-making increasingly depend upon imaging tests. As in other medical fields, the accumulation of published literature in radiology has become the basis of evidence-based practice or evidence-based radiology. The rapid evolution of imaging technology places unique demands upon this research effort, for re-evaluation of reproducibility, diagnostic test accuracy, and comparative performance against existing imaging tests—in the setting of varying patient populations and techniques for each imaging test. Additionally, the current era of health-care policy, with its emphasis on not only efficacy and effectiveness, but also value, requires evidence about how imaging technology translates into qualitative and quantitative changes in health outcomes and efficiency of clinical care.
Value can be simply defined as the health outcomes achieved per dollar spent . Because of the concern that indiscriminate diagnostic imaging use contributes to high health-care costs and potentially lower quality of care, policies intended to encourage evidence-based use of imaging are being enacted. For example, the Centers for Medicare and Medicaid Services will require ordering physicians to consult appropriate use criteria for imaging tests such as those endorsed by national medical specialty societies, including the American College of Radiology, to avoid reimbursement deductions, and also requires documentation of shared decision-making with patients regarding the benefits and harms of lung cancer screening . In efforts to enhance quality and value in the health-care system, decision-makers from day-to-day practitioners to expert panels and policy-making bodies are evaluating evidence on the impact of diagnostic tests on health outcomes for patients and health-care systems.
The purpose of this article is to provide an overview of some of the methodological issues and approaches that bridge diagnostic test accuracy and health outcomes research: (1) how to determine when a diagnostic test merits further evaluation, (2) when study of surrogate outcomes can be useful, (3) how to consider the possible harms as well as potential benefits of a test, and (4) how to integrate evidence of an imaging test’s efficacy/effectiveness with clinical data to assess outcomes and value.
When Does a Diagnostic Test Merit Further Evaluation through Outcomes Research?
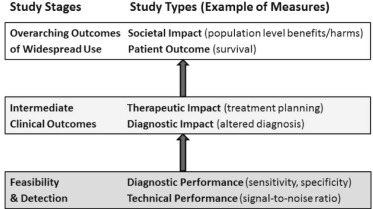
The assessment of imaging tests encompasses several stages, and may be described as a hierarchy of study types, allproviding evidence in support of, and ideally before, a test’s widespread clinical adoption. At the top, patient outcomes (eg life expectancy) and societal impact (eg cost-effectiveness) capture the overarching effect of a diagnostic test on patients and align its use with the ideals of improved population health and sometimes, enhanced value over existing alternatives. In descending order, the study types in the hierarchy include therapeutic and diagnostic impact, diagnostic performance, and technical performance ( Fig 1 ) .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
When Is Study of Intermediate or Surrogate Outcomes Useful?
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Methodological Building Blocks of Outcomes Research: Investigation of Benefits and Harms
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Experimental Studies
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Observational Studies
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Meta-analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Benefits and Harms in Patient-reported Outcomes
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Integration of Efficacy/Effectiveness and Clinical Data to Assess Outcomes: Decision Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Porter M.E.: What is value in health care?. N Engl J Med 2010; 363: pp. 2477-2481.
2. H.R.4302 : Protecting access to Medicare Act of 2014. United States Congress website; Published April 4; Available at: https://www.congress.gov/bill/113th-congress/house-bill/4302 Accessed December 15, 2015
3. Decision memo for screening for lung cancer with low dose computed tomography. Centers for Medicare & Medicaid Services website; Published February 5; Available at: https://www.cms.gov/medicare-coverage-database/details/nca-decision-memo.aspx?NCAId=274 Accessed December 15, 2015
4. Sardanelli F., Hunink M.G., Gilbert F.J., et. al.: Evidence-based radiology: why and how?. Eur Radiol 2010; 20: pp. 1-15.
5. Fineberg H.V., Bauman R., Sosman M.: Computerized cranial tomography. Effect on diagnostic and therapeutic plans. JAMA 1977; 238: pp. 224-227.
6. Fryback D.G., Thornbury J.R.: The efficacy of diagnostic imaging. Med Decis Making 1991; 11: pp. 88-94.
7. Phelps C.E., Mushlin A.I.: Focusing technology assessment using medical decision theory. Med Decis Making 1988; 8: pp. 279-289.
8. Heijenbrok-Kal M.H., Buskens E., Nederkoorn P.J., et. al.: Optimal peak systolic velocity threshold at duplex us for determining the need for carotid endarterectomy: a decision analytic approach. Radiology 2006; 238: pp. 480-488.
9. Hassan C., Hunink M.G., Laghi A., et. al.: Value-of-information analysis to guide future research in colorectal cancer screening. Radiology 2009; 253: pp. 745-752.
10. Temple R.: Are surrogate markers adequate to assess cardiovascular disease drugs?. JAMA 1999; 282: pp. 790-795.
11. Fleming T.R., DeMets D.L.: Surrogate end points in clinical trials: are we being misled?. Ann Intern Med 1996; 125: pp. 605-613.
12. Johnson J.R., Ning Y.M., Farrell A., et. al.: Accelerated approval of oncology products: the food and drug administration experience. J Natl Cancer Inst 2011; 103: pp. 636-644.
13. Marmot M.G., Altman D.G., Cameron D.A., et. al.: The benefits and harms of breast cancer screening: an independent review. Br J Cancer 2013; 108: pp. 2205-2240.
14. Jarvik J.G., Hollingworth W., Martin B., et. al.: Rapid magnetic resonance imaging vs radiographs for patients with low back pain: a randomized controlled trial. JAMA 2003; 289: pp. 2810-2818.
15. Genders T.S., Meijboom W.B., Meijs M.F., et. al.: CT coronary angiography in patients suspected of having coronary artery disease: decision making from various perspectives in the face of uncertainty. Radiology 2009; 253: pp. 734-744.
16. Genders T.S., Steyerberg E.W., Hunink M.G., et. al.: Prediction model to estimate presence of coronary artery disease: retrospective pooled analysis of existing cohorts. BMJ 2012; 344: pp. e3485.
17. Godwin M., Ruhland L., Casson I., et. al.: Pragmatic controlled clinical trials in primary care: the struggle between external and internal validity. BMC Med Res Methodol 2003; 3: pp. 28.
18. Henderson D.R., de Souza N.M., Thomas K., et. al.: Nine-year follow-up for a study of diffusion-weighted magnetic resonance imaging in a prospective prostate cancer active surveillance cohort. Eur Urol 2015; Oct 1. pii: S0302-2838(15)00980-X6; Epub ahead of print
19. Midgette A.S., Stukel T.A., Littenberg B.: A meta-analytic method for summarizing diagnostic test performances: receiver-operating-characteristic-summary point estimates. Med Decis Making 1993; 13: pp. 253-257.
20. Kang S.K., Zhang A., Pandharipande P.V., et. al.: DWI for renal mass characterization: systematic review and meta-analysis of diagnostic test performance. AJR Am J Roentgenol 2015; 205: pp. 317-324.
21. Kierans A.S., Kang S.K., Rosenkrantz A.B.: The diagnostic performance of dynamic contrast-enhanced MR imaging for detection of small hepatocellular carcinoma measuring up to 2 cm: a meta-analysis. Radiology 2015; 278: pp. 82-94.
22. Smailagic N., Vacante M., Hyde C., et. al.: (1)(8)F-FDG PET for the early diagnosis of Alzheimer’s disease dementia and other dementias in people with mild cognitive impairment (MCI). Cochrane Database Syst Rev 2015; CD010632
23. Hulten E., Pickett C., Bittencourt M.S., et. al.: Outcomes after coronary computed tomography angiography in the emergency department: a systematic review and meta-analysis of randomized, controlled trials. J Am Coll Cardiol 2013; 61: pp. 880-892.
24. Goldstein J.A., Chinnaiyan K.M., Abidov A., et. al.: The CT-STAT (Coronary Computed Tomographic Angiography for Systematic Triage of Acute Chest Pain Patients to Treatment) trial. J Am Coll Cardiol 2011; 58: pp. 1414-1422.
25. Hoffmann U., Truong Q.A., Schoenfeld D.A., et. al.: Coronary CT angiography versus standard evaluation in acute chest pain. N Engl J Med 2012; 367: pp. 299-308.
26. Goldstein J.A., Gallagher M.J., O’Neill W.W., et. al.: A randomized controlled trial of multi-slice coronary computed tomography for evaluation of acute chest pain. J Am Coll Cardiol 2007; 49: pp. 863-871.
27. Higgins J.P., Thompson S.G.: Quantifying heterogeneity in a meta-analysis. Stat Med 2002; 21: pp. 1539-1558.
28. President’s Council of Advisors on Science and Technology : Priorities for personalized medicine.2008.President’s Council of Advisors on Science and TechnologyWashington, DC
29. U.S. Food and Drug Administration : Paving the way for personalized medicine: FDA’s role in a new era of medical product development. U.S. Food and Drug Administration website; Published October; Available at: http://www.fda.gov/downloads/ScienceResearch/SpecialTopics/PersonalizedMedicine/UCM372421.pdf Accessed April 24, 2015
30. Lerman C., Trock B., Rimer B.K., et. al.: Psychological and behavioral implications of abnormal mammograms. Ann Intern Med 1991; 114: pp. 657-661.
31. Brewer N.T., Salz T., Lillie S.E.: Systematic review: the long-term effects of false-positive mammograms. Ann Intern Med 2007; 146: pp. 502-510.
32. Tosteson A.N., Fryback D.G., Hammond C.S., et. al.: Consequences of false-positive screening mammograms. JAMA Intern Med 2014; 174: pp. 954-961.
33. Zigmond A.S., Snaith R.P.: The hospital anxiety and depression scale. Acta Psychiatr Scand 1983; 67: pp. 361-370.
34. Mushlin A.I., Kern L.M., Paris M., et. al.: The value of diagnostic information to patients with chest pain suggestive of coronary artery disease. Med Decis Making 2005; 25: pp. 149-157.
35. Swan J.S., Kong C.Y., Hur C., et. al.: Comparing morbidities of testing with a new index: screening colonoscopy versus core-needle breast biopsy. J Am Coll Radiol 2015; 12: pp. 295-301.
36. Humphrey K.L., Lee J.M., Donelan K., et. al.: Percutaneous breast biopsy: effect on short-term quality of life. Radiology 2014; 270: pp. 362-368.
37. Weinstein M.C., Fineberg H.V., Elstein A.S., et. al.: Clinical decision analysis.1980.SaundersPhiladelphia, PA
38. Kriza C., Emmert M., Wahlster P., et. al.: An international review of the main cost-effectiveness drivers of virtual colonography versus conventional colonoscopy for colorectal cancer screening: is the tide changing due to adherence?. Eur J Radiol 2013; 82: pp. e629-e636.
39. Beck J.R., Pauker S.G.: The Markov process in medical prognosis. Med Decis Making 1983; 3: pp. 419-458.
40. Beck J.R., Pauker S.G., Gottlieb J.E., et. al.: A convenient approximation of life expectancy (the “DEALE”). II. Use in medical decision-making. Am J Med 1982; 73: pp. 889-897.
41. Braithwaite R.S., Roberts M.S., Justice A.C.: Incorporating quality of evidence into decision analytic modeling. Ann Intern Med 2007; 146: pp. 133-141.
42. Cronin K.A., Legler J.M., Etzioni R.D.: Assessing uncertainty in microsimulation modelling with application to cancer screening interventions. Stat Med 1998; 17: pp. 2509-2523.
43. Groot Koerkamp B., Weinstein M.C., Stijnen T., et. al.: Uncertainty and patient heterogeneity in medical decision models. Med Decis Making 2010; 30: pp. 194-205.
44. Weinstein M.C., Siegel J.E., Gold M.R., et. al.: Recommendations of the panel on cost-effectiveness in health and medicine. JAMA 1996; 276: pp. 1253-1258.
45. Lee C.I., Cevik M., Alagoz O., et. al.: Comparative effectiveness of combined digital mammography and tomosynthesis screening for women with dense breasts. Radiology 2015; 274: pp. 772-780.
46. Weinstein M.C., O’Brien B., Hornberger J., et. al.: Principles of good practice for decision analytic modeling in health-care evaluation: report of the ISPOR Task Force on Good Research Practices–Modeling Studies. Value Health 2003; 6: pp. 9-17.