
Rationale and Objectives
Pulmonary nodules can be missed on the non-breath hold computed tomography (CT) portion of 18F-fluorodeoxyglucose positron emission tomography/computed tomography (FDG PET/CT), and for this reason prior studies have advocated for routinely performing dedicated breath hold CT of the chest in addition to PET/CT for routine staging of malignancy. We evaluated the rate of pulmonary nodule detection on standard CT images from whole body PET/CT studies (WB-PET/CT), high-resolution lung reconstruction CT images from PET/CT studies (HR-PET/CT), and diagnostic breath hold chest CT (BH-CT).
Materials and Methods
A cohort of 25 patients was identified who had a history of lung cancer as well as a PET/CT staging or restaging scan and BH-CT within 30 days of each other. All PET/CTs included a set of CT images using a soft tissue algorithm filter and 3.75- to 5-mm slice thickness, as well as high-resolution reformats with a sharp reconstruction filter and 2-mm slice thickness. The CT images from WB-PET/CT, HR-PET/CT, and BH-CT were reviewed by three radiologists. Significance was analyzed by two-way repeated measures analysis of variance.
Results
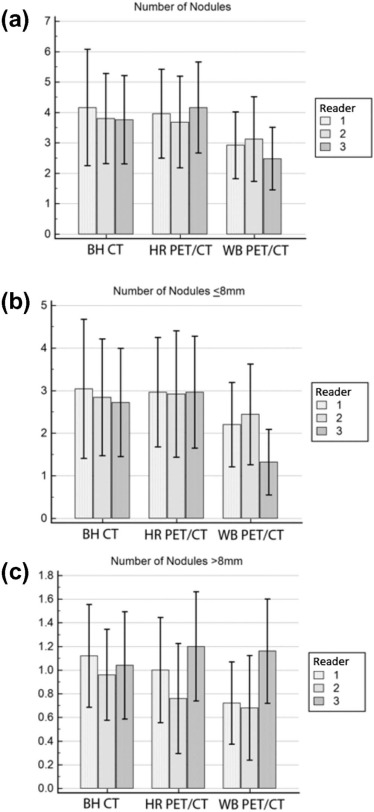
There were 2.84 nodules found per patient with WB-PET/CT, 3.85 nodules with HR-PET/CT, and 3.91 nodules with BH-CT. When only nodules less than or equal to 8 mm in size were considered, WB-PET/CT also demonstrated significantly fewer nodules (1.98) compared to the HR-PET/CT (2.94) or a BH-CT (2.86) ( P < 0.001). No difference in detection rate was noted between the two higher resolution modalities.
Conclusions
More pulmonary nodules are detected on the CT portion of PET/CT studies when high-resolution reformatted images are created and reviewed. The ability to detect nodules with the reformatted images was indistinguishable from dedicated BH-CT. Overall, high-resolution reformats of PET/CT images of the lungs can increase the sensitivity for pulmonary nodule detection, approaching that of dedicated BH-CT. These data suggest that if HR-PET/CT reformats are used, additional dedicated BH-CT is unnecessary for routine staging of lung cancer.
Introduction
8F-Fluorodeoxyglucose (FDG) positron emission tomography combined with whole body computed tomography (PET/CT) has become the standard of care imaging test for staging of patients with non-small cell lung cancer (NSCLC) . Staging of NSCLC is performed using the tumor, node, metastasis (TNM) classification system . Multiple prior studies have demonstrated that PET/CT is superior to CT alone for staging the primary mass (T stage) , associated nodal disease (N stage) , and distant metastasis (M stage) . For these reasons, PET/CT has become widely used for this application.
The presence or absence of pulmonary nodules, distinct from the primary mass, is an important contributor to the overall stage of NSCLC . Specifically, the presence of other nodules in the same lobe as the primary tumor confers the T3 stage, and the presence of nodules in the same side, different lobe, results in a T4 tumor. Metastatic pulmonary nodules in the contralateral lung confer M1a disease. An accurateassessment for nodules suggestive of metastatic disease can only be accomplished via imaging; therefore, it is critical to accurately assess the presence of even small pulmonary nodules.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Methods
Patient Selection
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Scan Technique
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Imaging and Chart Review
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Patient Demographics
Get Radiology Tree app to read full this article<
TABLE 1
Patient Demographics
Age 70.3 ± 7.2 years Sex Male 14/25 (56%) Female 11/25 (44%) Average time between PET and CT scan 17.8 ± 8.0 days Indication for CT Restaging/treatment response/surveillance 19/25(76%) Initial staging 4/25(16%) Suspected pulmonary embolism 2/25(8%) Indication for PET/CT Restaging/treatment response/surveillance 21/25(86%) Initial staging 4/25(16%)
PET/CT, positron emission tomography/computed tomography.
Get Radiology Tree app to read full this article<
Scan Interpretation
Get Radiology Tree app to read full this article<
![Figure 1, Examples of pulmonary nodules detected using various methods. ( a ) A 67-year-old man with history of non-small cell lung cancer (NSCLC) post-resection with a 4-mm nodule found along the suture line. The nodule was detected on whole body positron emission tomography/computed tomography (WB-PET/CT) by one out of three radiologists, on high-resolution PET/CT (HR-PET/CT) by three out of three radiologists, and on breath hold chest CT (BH-CT) by three out of three radiologists. ( b ) A 67-year-old man with history of NSCLC post-resection (same patient as [ a ] with a 4-mm left lower lobe pulmonary nodule). The nodule was detected on WB-PET/CT by one of three radiologists, on HR-PET/CT by three out of three radiologists, and on BH-CT by three out of three radiologists. ( c ) A 78-year-old woman with history of NSCLC with recurrence. Images demonstrate a 3-mm subpleural right upper lobe nodule, detected on WB-PET/CT by none of three radiologists, on HR-PET/CT by two out of three radiologists, and on BH-CT by two out of three radiologists.](https://storage.googleapis.com/dl.dentistrykey.com/clinical/DetectingPulmonaryNodulesinLungCancerPatientsUsingWholeBodyFDGPETCTHighresolutionLungReformatofFDGPETCTorDiagnosticBreathHoldChestCT/0_1s20S1076633216300769.jpg)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Kligerman S., Digumarthy S.: Staging of non-small cell lung cancer using integrated PET/CT. AJR Am J Roentgenol 2009; 193: pp. 1203-1211.
2. UyBico S.J., Wu C.C., Suh R.D., et. al.: Lung cancer staging essentials: the new TNM staging system and potential imaging pitfalls. Radiographics 2010; 30: pp. 1163-1181.
3. Rami-Porta R., Ball D., Crowley J., et. al.: The IASLC Lung Cancer Staging Project: proposals for the revision of the T descriptors in the forthcoming (seventh) edition of the TNM classification for lung cancer. J Thorac Oncol 2007; 2: pp. 593-602.
4. Postmus P.E., Brambilla E., Chansky K., et. al.: The IASLC Lung Cancer Staging Project: proposals for revision of the M descriptors in the forthcoming (seventh) edition of the TNM classification of lung cancer. J Thorac Oncol 2007; 2: pp. 686-693.
5. Goldstraw P., Crowley J., Chansky K., et. al.: The IASLC Lung Cancer Staging Project: proposals for the revision of the TNM stage groupings in the forthcoming (seventh) edition of the TNM classification of malignant tumours. J Thorac Oncol 2007; 2: pp. 706-714.
6. De Wever W., Stroobants S., Coolen J., et. al.: Integrated PET/CT in the staging of nonsmall cell lung cancer: technical aspects and clinical integration. Eur Respir J 2009; 33: pp. 201-212.
7. Cerfolio R.J., Ojha B., Bryant A.S., et. al.: The accuracy of integrated PET-CT compared with dedicated PET alone for the staging of patients with nonsmall cell lung cancer. Ann Thorac Surg 2004; 78: pp. 1017-1023. discussion 1017–1023
8. Schrevens L., Lorent N., Dooms C., et. al.: The role of PET scan in diagnosis, staging, and management of non-small cell lung cancer. Oncologist 2004; 9: pp. 633-643.
9. Thipphavong S., Lim R., Zabor E., et. al.: Clinical significance of pulmonary nodules missed on non-breath-hold PET/CT. J Nucl Med Radiat Ther 2013; 4: pp. 159.
10. Allen-Auerbach M., Yeom K., Park J., et. al.: Standard PET/CT of the chest during shallow breathing is inadequate for comprehensive staging of lung cancer. J Nucl Med 2006; 47: pp. 298-301.
11. Juergens K.U., Weckesser M., Stegger L., et. al.: Tumor staging using whole-body high-resolution 16-channel PET-CT: does additional low-dose chest CT in inspiration improve the detection of solitary pulmonary nodules?. Eur Radiol 2006; 16: pp. 1131-1137.
12. Aquino S.L., Kuester L.B., Muse V.V., et. al.: Accuracy of transmission CT and FDG-PET in the detection of small pulmonary nodules with integrated PET/CT. Eur J Nucl Med Mol Imaging 2006; 33: pp. 692-696.
13. Nomori H., Watanabe K., Ohtsuka T., et. al.: Evaluation of F-18 fluorodeoxyglucose (FDG) PET scanning for pulmonary nodules less than 3 cm in diameter, with special reference to the CT images. Lung Cancer 2004; 45: pp. 19-27.
14. Khalaf M., Abdel-Nabi H., Baker J., et. al.: Relation between nodule size and 18F-FDG-PET SUV for malignant and benign pulmonary nodules. J Hematol Oncol 2008; 1: pp. 13.
15. Fischbach F., Knollmann F., Griesshaber V., et. al.: Detection of pulmonary nodules by multislice computed tomography: improved detection rate with reduced slice thickness. Eur Radiol 2003; 13: pp. 2378-2383.
16. Takashima S., Sone S., Li F., et. al.: Small solitary pulmonary nodules (< or =1 cm) detected at population-based CT screening for lung cancer: reliable high-resolution CT features of benign lesions. AJR Am J Roentgenol 2003; 180: pp. 955-964.
17. Huang J.Y., Bristow B., Shafir S., et. al.: Coccidioidomycosis-associated deaths, United States, 1990–2008. Emerg Infect Dis 2012; 18: pp. 1723-1728.
18. Goerres G.W., Burger C., Kamel E., et. al.: Respiration-induced attenuation artifact at PET/CT: technical considerations. Radiology 2003; 226: pp. 906-910.
19. Chatziioannou S.N., Georgakopoulos A.T., Pianou N.K., et. al.: Recurrent thyroid cancer diagnosis: ROC study of the effect of a high-resolution head and neck 18F-FDG PET/CT scan. Acad Radiol 2014; 21: pp. 58-63.
20. Keogan M.T., Tung K.T., Kaplan D.K., et. al.: The significance of pulmonary nodules detected on CT staging for lung cancer. Clin Radiol 1993; 48: pp. 94-96.
21. Munden R.F., Pugatch R.D., Liptay M.J., et. al.: Small pulmonary lesions detected at CT: clinical importance. Radiology 1997; 202: pp. 105-110.
22. Ginsberg M.S., Griff S.K., Go B.D., et. al.: Pulmonary nodules resected at video-assisted thoracoscopic surgery: etiology in 426 patients. Radiology 1999; 213: pp. 277-282.
23. Kim Y.H., Lee K.S., Primack S.L., et. al.: Small pulmonary nodules on CT accompanying surgically resectable lung cancer: likelihood of malignancy. J Thorac Imaging 2002; 17: pp. 40-46.