
Rationale and Objectives
To determine the diagnostic accuracy of 64-row multidetector cardiac computed tomography (MDCT) in detecting aortic regurgitation (AR) on prospectively acquired images with trans-thoracic echocardiography (TTE) as a reference standard.
Materials and Methods
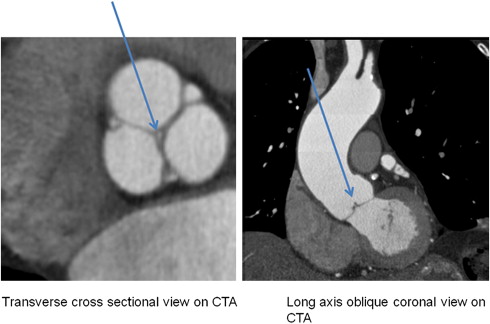
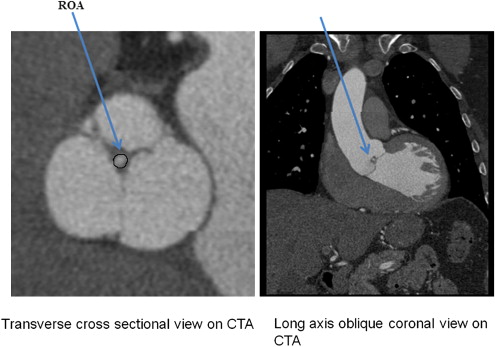
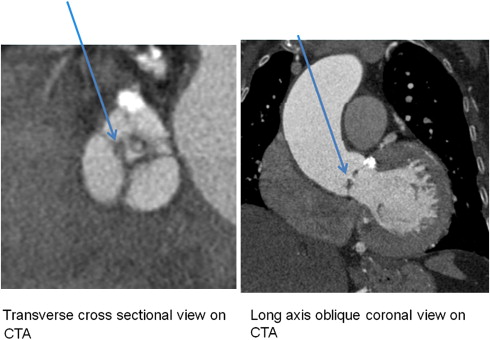
Forty-three consecutive patients underwent MDCT and TTE. AR was defined on MDCT images acquired at 75% phase of R-R interval as the lack of aortic cusps coaptation. The maximum regurgitant orifice area (ROA) was planimetered and compared to TTE.
Results
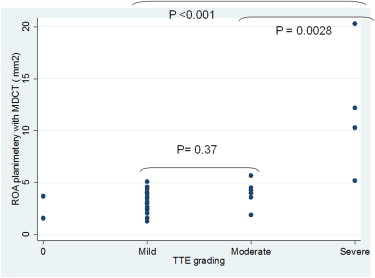
All 29 patients with AR on TTE were correctly identified by MDCT. The sensitivity, specificity, positive predictive value, and negative predictive value of MDCT were 100%, 85.7%, 93.5%, and 100%, respectively. Sixteen, nine, and four patients were found to have mild, moderate, and severe AR on TTE, respectively. The corresponding ROA by MDCT were 3.25 ± 1.04 mm 2 , 4.16 ± 1.19 mm 2 , and 11.30 ± 6.13 mm 2 , respectively.
Conclusion
MDCT data acquired for the coronary artery evaluation can be used for the detection of aortic regurgitation with high diagnostic accuracy without additional scanning or radiation and can support appropriate referral for TTE.
Aortic regurgitation (AR) is a common clinical condition, with increasing prevalence as the population ages. The overall prevalence of AR was 4.9% in the Framingham Heart study and 10% in the Strong Heart Study . Clinically, patients with AR can remain asymptomatic and undetected for a long time . Significant left ventricular decompensation may accompany the initial diagnosis. Cardiac auscultation can reveal the characteristic murmur and patients can be referred for echocardiography for confirmation. Trans-thoracic echocardiography (TTE) not only confirms the presence of AR, but also determines its etiology, severity, and the effects of the regurgitant lesion on left ventricular size and function .
Currently the utilization of multidetector cardiac computed tomography (MDCT) has increased for the detection of coronary artery disease . With increased temporal and spatial resolution, it is now possible to perform detailed evaluation of various noncoronary cardiac structures. Multiple clinical studies have shown the role of MDCT in detecting mitral regurgitation as well as aortic stenosis .
Get Radiology Tree app to read full this article<
Materials and methods
Study Population
Get Radiology Tree app to read full this article<
MDCT Image Acquisition and Postprocessing
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
MDCT Image Reconstruction and Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
TTE
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
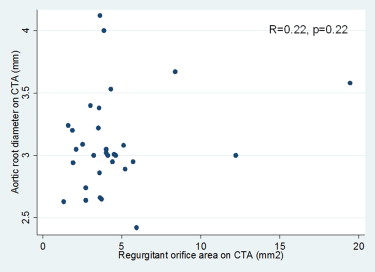
Table 1
Patient Characteristics
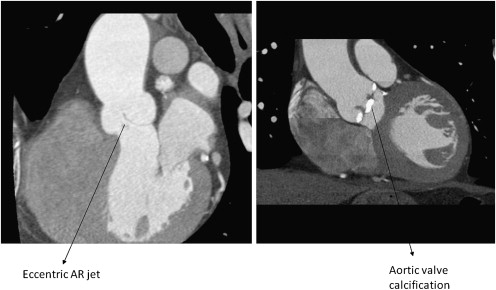
Characteristics ( n = 43) Mean ± SD OR No. (%) Age (y) 64.5 ± 16 Male 25 (58.14) Hypertension 16 (55.17) Diabetes mellitus 5 (13) Hyperlipidemia 17 (42.5) AVC score on CT(AU) ( n = 16) 30.56 ± 93.45 History of CAD 20 (51.28) Ejection fraction on TTE 54.26 ± 12.71 Prevalence of AR by echo 29 (67.44) Aortic root diameter on CTA (mm) 3.45 ± 0.391 Aortic valve morphology Tricuspid 41 (95.35) Bicuspid 1 (2.33) Quadricuspid 1 (2.33) AR jet position Central 30 (96.7) Eccentric 1 (3.3) Heart rate at the time of CTA (beats/min) 55 ± 7.5 (range, 38–73) Time duration between TTE and CTA (days) 59.3 ± 55.4 (range, 0–180)
TTE, trans-thoracic echocardiography; CTA, computed tomography angiogram; AU, Agatston units; AR, aortic regurgitation; AVC, aortic valve calcium; CAD, coronary artery disease.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Correlation of Severity of AR on Echo with Aortic Regurgitation Orifice Area on CTA
Severity of AR on TTE No. of Patients Mean ROA on CTA (mm 2 ) Range (mm 2 ) Standard Deviation 95% Confidence Interval Mild 16 3.25 1.3–5.1 1.04 2.69–3.80 Moderate 9 4.16 1.9–5.92 1.19 3.24–5.08 Severe 4 11.30 5.2–19.45 6.13 1.53–21.07
TTE, trans-thoracic echocardiography; ROA, regurgitation orifice area; AR, aortic regurgitation; CTA, computed tomography angiography.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Limitations
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
References
1. Singh J.P., Evans J.C., Levy D., et. al.: Prevalence and clinical determinants of mitral, tricuspid, and aortic regurgitation (the Framingham Heart Study). Am J Cardiol 1999; 83: pp. 897-902. Erratum in: Am J Cardiol 1999;84:1143
2. Lebowitz N.E., Bella J.N., Roman M.J., et. al.: Prevalence and correlates of aortic regurgitation in American Indians: the Strong Heart Study. J Am Coll Cardiol 2000; 36: pp. 461-467.
3. Bonow R.O., Carabello B., de Leon A.C., et. al.: Guidelines for the management of patients with valvular heart disease: executive summary. A report of the American College of Cardiology/American Heart Association Task force on Practice Guidelines (Committee on management of patients with valvular heart disease). Circulation 1998; 98: pp. 1949-1984.
4. Bekeredjian R., Grayburn P.A.: Valvular heart disease: aortic regurgitation. Circulation 2005; 112: pp. 125-134.
5. Enriquez-Sarano M., Tajik A.J.: Clinical practice: aortic regurgitation. N Engl J Med 2004; 351: pp. 1539-1546.
6. Zoghbi W.A., Enriquez-Sarano M., Foster E., et. al.: Recommendations for evaluation of the severity of native valvular regurgitation with two-dimensional and Doppler echocardiography. J Am Soc Echocardiogr 2003; 16: pp. 777-802.
7. Leber A.W., Knez A., von Ziegler F., et. al.: Quantification of obstructive and nonobstructive coronary lesions by 64-slice computed tomography: a comparative study with quantitative coronary angiography and intravascular ultrasound. J Am Coll Cardiol 2005; 46: pp. 147-154.
8. Alkadhi H., Wildermuth S., Plass A., et. al.: Aortic stenosis: comparative evaluation of 16-detector row CT and echocardiography. Radiology 2006; 240: pp. 47-55.
9. Feuchtner G.M., Dichtl W., Friedrich G.J., et. al.: Multislice computed tomography for detection of patients with aortic valve stenosis and quantification of severity. J Am Coll Cardiol 2006; 47: pp. 1410-1417.
10. Bouvier E., Logeart D., Sablayrolles J.L., et. al.: Diagnosis of aortic valvular stenosis by multislice cardiac computed tomography. Eur Heart J 2006; 27: pp. 3033-3038.
11. Alkadhi H., Wildermuth S., Bettex D.A., et. al.: Mitral regurgitation: quantification with 16-detector row CT—initial experience. Radiology 2006; 238: pp. 454-463.
12. Feuchtner G.M., Dichtl W., Schachner T., et. al.: Diagnostic performance of MDCT for detecting aortic valve regurgitation. AJR Am J Roentgenol 2006; 186: pp. 1676-1681.
13. Jassal D.S., Shapiro M.D., Neilan T.G., et. al.: 64-slice multidetector computed tomography (MDCT) for detection of aortic regurgitation and quantification of severity. Invest Radiol 2007; 42: pp. 507-512.
14. Alkadhi H., Desbiolles L., Husmann L., et. al.: Aortic regurgitation: assessment with 64-section CT. Radiology 2007; 245: pp. 111-121.
15. Feuchtner G.M., Dichti W., Muller S., et. al.: 64- MDCT for diagnosis of aortic regurgitation in patients referred to CT coronary angiography. AJR Am J Roentgenol 2008; 191: pp. W1-W7.
16. Li X., Tang L., Zhou L., et. al.: Aortic valves stenosis and regurgitation: assessment with dual source computed tomography. Int J Cardiovasc Imaging 2009; 25: pp. 591-600.
17. Gopal A., Mao S.S., Karlsberg D., et. al.: Radiation reduction with prospective ECG-triggering acquisition using 64-multidetector computed tomographic angiography. Int J Cardiovasc Imaging 2009; 25: pp. 405-416.
18. Gopal A., Budoff M.J.: A new method to reduce radiation exposure during multi-row detector cardiac computed tomographic angiography. Int J Cardiol 2009; 132: pp. 435-436.
19. Isma’eel H., Hamirani Y.S., Mehrinfar R., et. al.: Optimal phase for coronary interpretations and correlation of ejection fraction using late-diastole and end-diastole imaging in cardiac computed tomography angiography: implications for prospective triggering. Int J Cardiovasc Imaging 2009; 25: pp. 739-749.
20. Budoff M.J.: Maximizing dose reductions with cardiac CT. Int J Cardiovasc Imaging 2009; 25: pp. 279-287.
21. Budoff M.J., Achenbach S., Blumenthal R.S., et. al.: Assessment of coronary artery disease by cardiac computed tomography, a scientific statement from the American Heart Association Committee on Cardiovascular Imaging and Intervention, Council on Cardiovascular Radiology and Intervention, and Committee on Cardiac Imaging, Council on Clinical Cardiology. Circulation 2006; 114: pp. 1761-1791.