
Rationale and Objectives
To evaluate the sensitivity of high-resolution breast-specific gamma imaging (BSGI) for the detection of ductal carcinoma in situ (DCIS) based on histopathology and to compare the sensitivity of BSGI with mammography and magnetic resonance imaging (MRI) for the detection of DCIS.
Materials and Methods
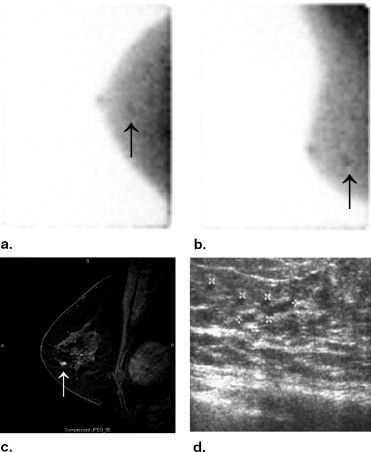
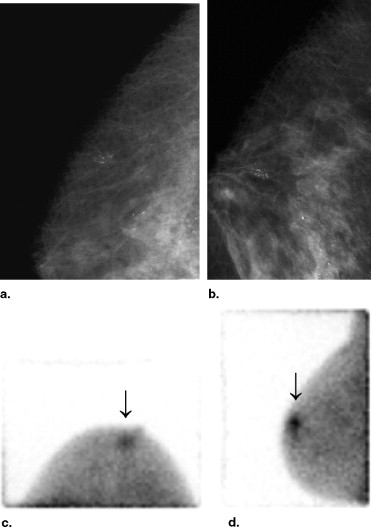
Twenty women, mean 55 years (range 34–76 years), with 22 biopsy-proven DCIS were retrospectively reviewed. After injection of 25–30 mCi (925–1,110 MBq) technetium 99m-sestamibi, patients had BSGI with a high-resolution, small-field-of-view gamma camera in craniocaudal and mediolateral oblique projections. BSGI studies were prospectively classified according to focal radiotracer uptake using a 1 to 5 scale, as normal 1), with no focal or diffuse uptake; benign 2), with minimal patchy uptake; probably benign 3), with scattered patchy uptake; probably abnormal 4), with mild focal radiotracer uptake; and abnormal 5), with marked focal radiotracer uptake. Imaging findings were compared to findings at biopsy or surgical excision. The sensitivity of BSGI, mammography, and when performed, MRI were determined for the detection of DCIS. Breast MRI was performed on seven patients with eight biopsy-proven foci. The sensitivities were compared using a two-tailed t -test and confidence intervals were determined.
Results
Pathologic tumor size of the DCIS ranged from 2 to 21 mm (mean 9.9 mm). Of 22 cases of biopsy-proven DCIS in 20 women, 91% were detected with BSGI, 82% were detected with mammography, and 88% were detected with magnetic resonance imaging. BSGI had the highest sensitivity for the detection of DCIS, although this small sample size did not demonstrate a statistically significant difference. Two cases of DCIS (9%) were diagnosed only after BSGI demonstrated an occult focus of radiotracer uptake in the contralateral breast, previously undetected by mammography. There were two false-negative BSGI studies
Conclusions
BSGI has higher sensitivity for the detection of DCIS than mammography or MRI and can reliably detect small, subcentimeter lesions.
Ductal carcinoma in situ (DCIS) occurs in approximately 28% or more than 58,000 cases of breast cancer in the United States ( ). Mammography, the only accepted screening tool for breast cancer, detects the majority of clinically occult DCIS as microcalcifications, the hallmark mammographic finding of DCIS ( ). Yet, the diagnosis of DCIS remains difficult because mammography is unreliable in predicting the histology and extent of DCIS (2–5).
Breast MRI has been shown to have a sensitivity of 73%–89% for DCIS, but a limited specificity (58%–89%) and variable positive predictive value (25%–84%) ( ). As with mammography, small foci of DCIS are difficult to detect on magnetic resonance imaging (MRI), particularly lesions smaller than 5 mm ( ). In addition, MRI may overestimate DCIS extent in as many as 50% of cases and often cannot distinguish benign from malignant lesions, high-grade from low-grade DCIS, or detect an invasive component concurrent with the DCIS (3–5). As a result, MRI remains a secondary study with limitations in DCIS detection and evaluation.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
BSGI versus Mammography
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
BSGI versus MRI
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Two-Tailed t -test Evaluating Sensitivity of Breast-Specific Gamma Imaging (BSGI) to Mammography and Magnetic Resonance Imaging (MRI)
Contrast Value of Contrast Standard Error_t_ df_P_ Value (BSGI to mammography) 0.09 0.105 0.864 49 .392 (BSGI to MRI) 0.03 0.144 0.237 49 .814
Table 2
Confidence Intervals
Imaging Modality 95% Confidence Intervals Breast-specific gamma imaging (n = 22) 0.78–1.04 Mammography (n = 22) 0.64–0.99 Magnetic resonance imaging (n = 8) 0.58–1.17
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Jemal A., Murray T., Ward E., et. al.: Cancer statistics 2005. CA Cancer J Clin 2005; 55: pp. 10-30.
2. Burstein H.J., Polyak K., Wong J.S., et. al.: Ductal carcinoma in situ of the breast. N Engl J Med 2004; 350: pp. 1430-1441.
3. Bluemke D.A., Gatsonis C.A., Chen M.H., et. al.: Magnetic resonance imaging of the breast prior to biopsy. JAMA 2004; 22: pp. 2735-2742.
4. Hwang E.S., Kinkel K., Esserman L.J., et. al.: Magnetic resonance imaging in patients diagnosed with ductal carcinoma-in-situ: value in the diagnosis of residual disease, occult invasion, and multicentricity. Ann Surg Oncol 2003; 10: pp. 381-388.
5. Orel S.G., Mendonca M.H., Reynolds C., et. al.: MR imaging of ductal carcinoma in situ. Radiology 1997; 202: pp. 413-420.
6. Taillefer R.: Clinical applications of 99mTc-sestamibi scintimammography. Semin Nucl Med 2005; 35: pp. 100-115.
7. Schillaci O., Buscombe J.R.: Breast scintigraphy today: indications and limitations. Eur J Nucl Med Mol Imaging 2004; 31: pp. S35-S45.
8. Khalkhali I., Cutrone J.A., Mena I.G., et. al.: Scintimammography: the complementary role of Tc99m sestamibi prone breast imaging for the diagnosis of breast carcinoma. Radiology 1995; 196: pp. 421-426.
9. Khalkhali I., Villanueva-Meyer J., Edell S.L., et. al.: Diagnostic accuracy of 99m Tc-Sestamibi breast imaging: multicenter trial results. J Nucl Med 2000; 41: pp. 1973-1979.
10. Papantoniou V., Tsiouris S., Mainta E., et. al.: Imaging in situ breast carcinoma (with or without an invasive component) with technetium-99m 20methoxy isobutyl isonitrile scintimammography. Breast Cancer Res 2005; 7: pp. R33-R45.
11. Ikeda D.M., Birdwell R.L., Daniel B.L.: Potential role of magnetic resonance imaging and other modalities in ductal carcinoma in situ detection. MRI Clin N Am 2001; 9: pp. 345-356.