
Rationale and Objectives
The aim of this study was to determine how often breast-specific gamma imaging (BSGI) identifies occult cancerous lesions in women with one suspicious lesion detected on mammography or physical exam.
Materials and Methods
A retrospective review was performed of the records of all patients who underwent BSGI between January 1, 2004, and June 4, 2007. Included in the study were 159 women who had one suspicious breast lesion on physical exam and/or mammography and who underwent BSGI to evaluate for occult lesions in the breast. All patients had one or more foci of cancer proven pathologically. BSGI findings were classified as normal or abnormal on the basis of the presence of focal radiotracer uptake.
Results
BSGI detected additional suspicious lesions occult to mammography and physical exam in 46 of 159 women (29%). BSGI identified occult cancer in 14 of 40 women (35%) who underwent biopsy or excision because of BSGI findings and in 14 of the 159 (9%) women in this study. In nine women, the occult cancer was present in the same breast as the index lesion (6%), and in five women, the occult cancer was found in the contralateral breast (3%).
Conclusions
BSGI is an effective imaging modality in the identification of mammographically and clinically occult cancer in women with one suspicious breast lesion.
Breast conservation surgery has replaced mastectomy as the preferred treatment for early-stage breast cancer . However, when two or more primary tumors are located in different quadrants of the breast, breast-conserving therapy is contraindicated . Routine physical examinations and mammography are the most common methods for early cancer detection, but they have diagnostic limitations. A study of 282 mastectomy specimens (performed for unifocal breast cancer) found that 63% of breasts had additional sites of cancer not detected by clinical examination or mammography, including 7% with additional foci of cancer in a different quadrant of the breast . Additional analyses of the pathology of mastectomy specimens have shown sites of cancer other than the index lesion in 20% to 63% . To achieve the highest possible level of diagnostic accuracy in the preoperative radiologic assessment, additional imaging techniques may be used. These include ultrasound, magnetic resonance imaging (MRI), and breast-specific gamma imaging (BSGI). Ultrasound, the primary diagnostic adjunct to mammography, aids in the diagnostic evaluation of mammographic findings and is used to guide interventional procedures . Houssami et al reported sensitivity of 96% and specificity of 79% for the combination of mammography and breast ultrasound in the identification of breast cancer.
Although mammography and ultrasound are predominantly anatomic in their approach to breast cancer diagnosis, MRI and BSGI rely on physiologic changes for the evaluation of breast cancer. Molecular breast imaging, or BSGI, uses a high-resolution, small–field of view gamma camera specific to breast imaging , which has demonstrated improved sensitivity for the detection of breast cancer . The sensitivity of BSGI ranges from 78.6% to 100% for detecting breast cancer, which is comparable to that of MRI (73%–100%) . Breast MRI and BSGI are similar in their ability to detect intraductal cancer, with sensitivities reported ranging from 88% and 92% for breast MRI and 91% to 94% for BSGI . Additionally, both breast MRI and BSGI can detect breast cancers that are mammographically and clinically occult . BSGI can detect subcentimeter occult cancers as small as 1 mm . The reported specificities of BSGI and breast MRI are also similar, ranging from 59.5% to 93.3% for BSGI and from 37% to 97% for breast MRI . Although BSGI and MRI are similar in their ability to detect breast cancer, BSGI has advantages in ease of performing the examination for patients and in interpretation for radiologists. Although MRI may be difficult for patients with claustrophobia and not possible in patients with renal insufficiency, implantable devices, or large body habitus, BSGI can be performed in any woman with venous access. A breast MRI examination often generates >1000 images, compared to four to 10 images with BSGI, with a concomitant decrease in interpretation time. Although formal cost analysis studies are needed to further evaluate the relative costs, both the equipment and the cost of the study are lower with BSGI.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Subjects
Get Radiology Tree app to read full this article<
BSGI Technique and Interpretation
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Data Collection and Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Baseline Characteristics
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
BSGI-detected Additional Suspicious Lesions
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
BSGI-detected Occult Cancerous Lesions and Comparison with Index Lesion
Get Radiology Tree app to read full this article<
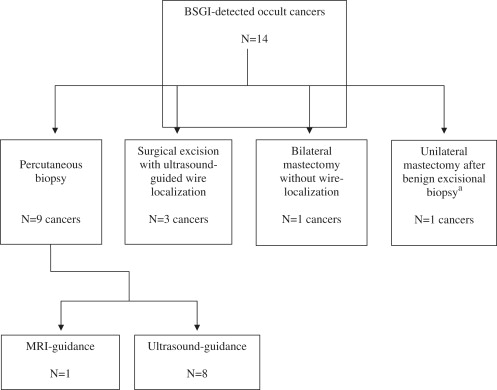
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Pathologic Features of BSGI-detected Occult Cancers
Pathology Total Frequency Contralateral Frequency Ipsilateral Frequency Infiltrating ductal carcinoma 6/14 (43%) 2/5 (40%) 4/9 (44%) Intermediate grade 3/6 High grade 3/6 Associated with DCIS 4/6 Infiltrating lobular carcinoma ∗ 3/14 (14%) 2/5 (40%) 1/9 (11%) Low grade 1/3 Associated with DCIS 1/3 DCIS 5/14 (36%) 1/5 (20%) 4/9 (44%) Low grade 1/5 Intermediate grade 1/5 High grade 3/5
BSGI, breast-specific gamma imaging; DCIS, ductal carcinoma in situ.
Get Radiology Tree app to read full this article<
Table 2
Sizes of BSGI-detected Occult Cancers
Size Description All Cancers Contralateral Cancers Ipsilateral Cancers Mean size of occult infiltrating cancers (cm) ∗ 1.16 0.58 1.6 Range of sizes of infiltrating cancers (cm) 0.15–3.6 0.15–1.0 0.8–3.6 Number of cancers <1 cm 7 † 4 † 3
BSGI, breast-specific gamma imaging.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Frequency of BSGI Detection of Occult Cancer Versus Various Parameters
Parameter Frequency of Detection_P_ Menopausal status Premenopausal 7/62 (11%) .38 Postmenopausal 7/97 (7%) Personal history of breast cancer Yes 1/19 (5%) 1 No 13/140 (9%) Family history of breast cancer Yes 7/68 (10%) .58 No 7/90 (8%) Breast density pattern 4 (extremely dense) 1/17 (6%) .74 ∗ 3 (heterogeneously dense) 9/98 (9%) 2 (scattered fibroglandular density) 4/33 (12%) 1 (almost entirely fat) 0/3 (0%) Pathology of index cancer Infiltrating lobular carcinoma 1/10 (10%) .25 ‡ Infiltrating ductal carcinoma 8/111 (7%) Infiltrating ductolobular carcinoma 1/3 (3%) Ductal carcinoma in situ 3/31 (10%) Other † 0/4 (0%) Size of index cancer § >0.2 cm 5/37 (14%) .29 <0.2 cm 5/75 (7%)
BSGI, breast-specific gamma imaging.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Fisher B., Redmond C., Poisson R., et. al.: Eight-year results of a randomized clinical trial comparing total mastectomy and lumpectomy with or without irradiation in the treatment of breast cancer. N Engl J Med 1989; 320: pp. 822-828.
2. Arriagada R., Le M.G., Rochard F., et. al.: Institut Gustave-Roussy Breast Cancer Group. Conservative treatment versus mastectomy in early breast cancer: patterns of failure with 15 years of follow-up data. J Clin Oncol 1996; 14: pp. 1558-1564.
3. Winchester D.P., Cox J.D.: Standards for breast-conservation treatment. CA Cancer J Clin 1992; 42: pp. 134-162.
4. Holland R., Veling S.H., Mravunac M., et. al.: Histologic multifocality of Tis, T1-2 breast carcinomas. Implications for clinical trials of breast-conserving surgery. Cancer 1985; 196: pp. 115-122.
5. Lagios M.D.: Multicentricity of breast carcinoma demonstrated by routine correlated serial subgross and radiographic examination. Cancer 1977; 40: pp. 1726-1734.
6. Schwartz G.F., Patchefsky A.S., Feig S.A., et. al.: Multicentricity of non-palpable breast cancer. Cancer 1980; 45: pp. 2913-2916.
7. Egan R.L.: Multicentric breast carcinomas: clinical-radiographic-pathologic whole organ studies and 10-year survival. Cancer 1982; 49: pp. 1123-1130.
8. Anastassiades O., Iakovou E., Stavridou N., et. al.: Multicentricity in breast cancer: a study of 366 cases. Am J Clin Pathol 1993; 99: pp. 238-243.
9. Vaidya J., Vyas J., Chinoy R., Merchant N., et. al.: Multicentricity in breast cancer: whole-organ analysis and clinical implications. Br J Cancer 1996; 74: pp. 820-824.
10. Zonderland H.M., Coerkamp E.G., Hermans J., et. al.: Diagnosis of breast cancer: contribution of US as an adjunct to mammography. Radiology 1999; 213: pp. 413-422.
11. American College of Radiology : ACR practice guideline for the performance of a breast ultrasound examination.2002.American College of RadiologyReston, VA:pp. 764-765.
12. Houssami N., Irwig L., Simpson J.M., et. al.: Sydney breast imaging accuracy study: comparative study of mammography and sonography in young women with symptoms. AJR Am J Roentgenol 2002; 180: pp. 935-940.
13. Majewski S., Kieper D., Curran E., et. al.: Optimization of dedicated scintimammography procedure using detector prototypes and compressible phantoms. IEEE Trans Nucl Sci 2001; 48: pp. 822-829.
14. Brem R.F., Kieper D.A., Rapelyea J.A.: Evaluation of a high-resolution, breast-specific, small-field-of-view gamma camera for the detection of breast cancer. Nucl Instrum Methods Phys Res A 2003; 497: pp. 39-45.
15. Brem R.F., Fishman M., Rapelyea J.A.: Detection of ductal carcinoma in situ with mammography, breast specific gamma imaging, and magnetic resonance imaging: a comparative study. Acad Radiol 2007; 14: pp. 945-950.
16. Bluemke D.A., Gatsonis C.A., Chen M.H., et. al.: Magnetic resonance imaging of the breast prior to biopsy. JAMA 2004; 292: pp. 2735-2742.
17. Brem R.F., Schoonjans J.M., Kieper D.A., et. al.: High-resolution scintimammography: a pilot study. J Nucl Med 2002; 43: pp. 909-915.
18. Brem R.F., Rapelyea J.A., Zisman G., et. al.: Occult breast cancer: scintimammography with high-resolution breast-specific gamma camera in women at high risk for breast cancer. Radiology 2005; 237: pp. 274-280.
19. Brem R.F., Floerke A.C., Rapelyea J.A., et. al.: Breast-specific gamma imaging as an adjunct imaging modality for the diagnosis of breast cancer. Radiology 2008; 247: pp. 651-657.
20. Kuhl C.K., Schrading S., Bieling H.B., et. al.: MRI for the diagnosis of pure ductal carcinoma in situ: a prospective observational study. Lancet 2007; 370: pp. 486-492.
21. Morris E.A., Liberman L., Ballon D.J., et. al.: MRI of occult breast carcinoma in a high-risk population. AJR Am J Roentgenol 2003; 181: pp. 619-626.
22. Orel S.G., Schnall M.D.: MR Imaging of the breast for the detection, diagnosis, and staging of breast cancer. Radiology 2001; 220: pp. 13-30.
23. Liberman L., Morris E.A., Kim C.A., et. al.: MR imaging findings in the contralateral breast of women with recently diagnosed breast cancer. AJR Am J Roentgenol 2003; 180: pp. 333-341.
24. Liberman L., Morris E.A., Dershaw D.D., et. al.: MR imaging of the ipsilateral breast in women with percutaneously proven breast cancer. AJR Am J Roentgenol 2003; 180: pp. 901-910.
25. Lee S.G., Orel S.G., Woo I.J., et. al.: MR imaging screening of the contralateral breast in patients with newly diagnosed breast cancer: preliminary results. Radiology 2003; 226: pp. 773-778.
26. Bartella L., Smith C.S., Dershaw D.D., et. al.: Imaging breast cancer. Radiol Clin N Am 2007; 45: pp. 45-67.
27. American College of Radiology : Breast Imaging Reporting and Data System (BI-RADS).3rd ed.1998.American College of RadiologyReston, VA
28. Coombs N.J., Boyages J.: Multifocal and multicentric breast cancer: does each focus matter?. J Clin Oncol 2005; 23: pp. 7497-7502.
29. Brem R.F., Ioffe M., Rapelyea J., et. al.: Invasive lobular carcinoma: detection with mammography, sonography, MRI, and breast-specific gamma imaging. AJR Am J Roentgenol 2009; 192: pp. 379-383.
30. Hungness E.S., Safa M., Shuaghnessy E.A., et. al.: Bilateral synchronous breast cancer: mode of detection and comparison of histologic features between the 2 breasts. Surgery 2000; 128: pp. 702-707.
31. LaTrenta L.R., Menell J.H., Morris E.A., et. al.: Breast lesion detected with MR imaging: utility and histopathologic importance of identification with ultrasound. Radiology 2003; 227: pp. 856-861.
32. Welch B., Brem R., Kross B., et. al.: Gamma-guided stereotactic breast biopsy system. IEEE Trans Nucl Sci 2006; 53: pp. 2690-2697.