
Rationale and Objectives
Prostate calcification is a noninvasive landmark for daily positioning of image-guided radiation therapy. However, detectability of prostate calcification with megavoltage helical computed tomography (MVCT) has not been evaluated. The purpose of this study was to evaluate the detectability of prostate calcification and to investigate how to predict detectability of calcification with MVCT.
Materials and Methods
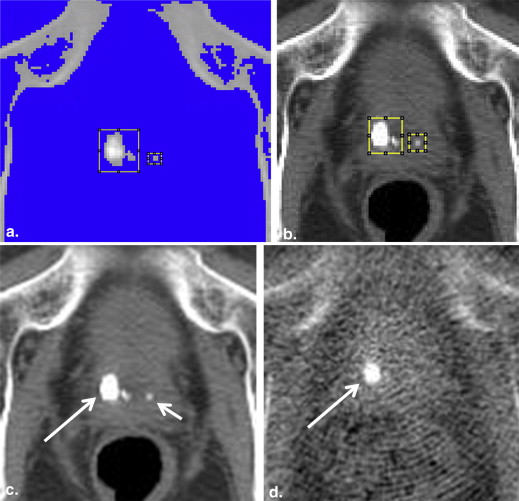
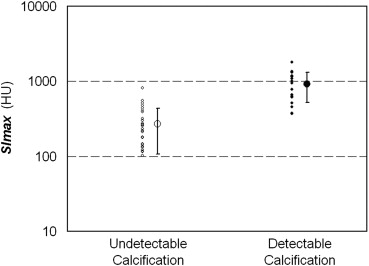
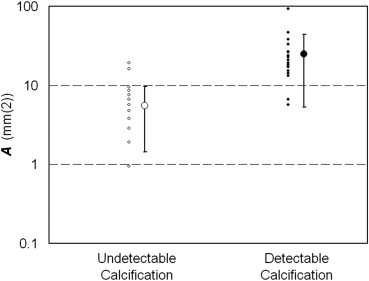
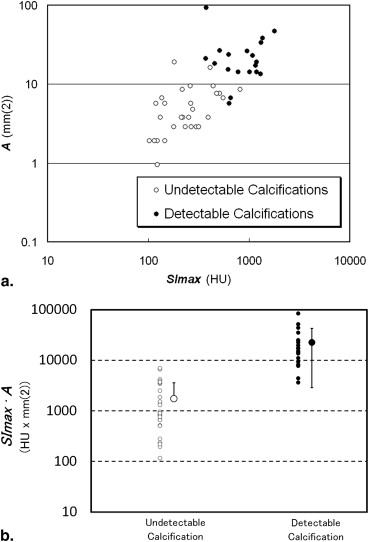
Thirty patients with prostate cancer who were scheduled for helical tomotherapy were included in this study. The detectability of prostate calcification on MVCT was evaluated by comparing against kilovoltage multidetector-row CT (KVCT) as the standard of reference. Maximum signal intensity ( SImax ), area ( A ) of calcification, and the product of both ( SImax·A ) were compared between undetectable and detectable calcifications. Then, the threshold values of SImax , A , and SImax·A were decided to achieve 100% sensitivity on MVCT.
Results
KVCT identified 49 calcifications in 28 of 30 patients. MVCT detected 19 (39%) of 49 calcifications in 15 (50%) of 30 patients. The minimum threshold values of SImax , A , and SImax·A to detect prostate calcifications were 953 HU, 20.98 mm 2 , and 7784 HU mm 2 , respectively. Using the threshold values of SImax , A , and SImax·A , 20% (10/49), 18% (9/49), and 35% (17/49) of calcifications were in the detection range, respectively.
Conclusions
MVCT can depict about one-third of prostate calcifications detectable on KVCT. The product of maximum signal intensity and area of calcification is the most distinguishable index for predicting patients showing prostate calcifications on MVCT.
Dose escalation with three-dimensional conformal radiotherapy or intensity-modulated radiation therapy (IMRT) for prostate cancer improves long-term prostate-specific antigen (PSA) control . The tight margins will decrease the volume dose delivered to organs at risk, but accurate positioning of the prostate is required for the high precision of planned radiotherapy treatments. Recent advancements in image-guided radiotherapy (IGRT) technologies provide the opportunity to localize target volumes with the same x-ray beam used for radiotherapy . Helical tomotherapy (HT) is an innovative means of delivering IGRT and IMRT using a device that combines features of a linear accelerator and a helical computed tomography (CT) scanner. HT is one of the successful innovative intensity-modulated IGRT techniques that can perform megavoltage CT (MVCT) scan and can obtain highly tailored dose distributions. MVCT enables imaging of anatomic structures in the presence of metallic dental or orthopedic implants. This is advantageous in cases with metal implants but has a limitation of reduced contrast in soft tissues . During HT of prostate cancer, prostate glands cannot always be clearly distinguished on MVCT. Thus, soft tissue matching for the prostate will be challenging in such cases.
Prostate calcifications are a common finding and seem mostly to be associated with benign prostatic hyperplasia. However, calcifications can occur in direct association with prostatic adenocarcinoma, although the incidence of this association is reported to be as low as 1.3% (4/298) . Physiological calcification has been considered to be a reliable landmark of the prostate position and allows for precise image guidance with low observation variations . However, the detectability of prostate calcifications with helical MVCT and the clinical application to HT has not yet been investigated. The purpose of this study was to determine the detection limit of prostate calcifications and to investigate whether calcification might be a natural landmark to localize the prostate during HT treatment.
Materials and methods
Study Population
Get Radiology Tree app to read full this article<
Imaging Protocol
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Calcification Scoring Method
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
References
1. Dearnaley D.P., Hall E., Lawrence D., et. al.: Phase III pilot study of dose escalation using conformal radiotherapy in prostate cancer: PSA control and side effects. Br J Cancer 2005; 92: pp. 488-498.
2. Kuban D.A., Tucker S.L., Dong L., et. al.: Long-term results of the M. D. Anderson randomized dose-escalation trial for prostate cancer. Int J Radiat Oncol Biol Phys 2008; 70: pp. 67-74.
3. Wong W.W., Vora S.A., Schild S.E., et. al.: Radiation dose escalation for localized prostate cancer: intensity-modulated radiotherapy versus permanent transperineal brachytherapy. Cancer 2009; 115: pp. 5596-5606.
4. Mackie T.R., Holmes T., Swerdloff S., et. al.: Tomotherapy: a new concept for the delivery of dynamic conformal radiotherapy. Med Phys 1993; 20: pp. 1709-1719.
5. Schubert L.K., Westerly D.C., Tomé W.A., et. al.: A comprehensive assessment by tumor site of patient setup using daily MVCT imaging from more than 3,800 helical tomotherapy treatments. Int J Radiat Oncol Biol Phys 2009; 73: pp. 1260-1269.
6. Sillanpaa J., Chang J., Mageras G., et. al.: Developments in megavoltage cone beam CT with an amorphous silicon EPID: reduction of exposure and synchronization with respiratory gating. Med Phys 2005; 32: pp. 819-829.
7. Beldjoudi G., Yartsev S., Bauman G., et. al.: Schedule for CT image guidance in treating prostate cancer with helical tomotherapy. Br J Radiol 2010; 83: pp. 241-251.
8. Sterzing F., Kalz J., Sroka-Perez G., et. al.: Megavoltage CT in helical tomotherapy—clinical advantages and limitations of special physical characteristics. Technol Cancer Res Treat 2009; 8: pp. 343-352.
9. Hong T.S., Welsh J.S., Ritter M.A., et. al.: Megavoltage computed tomography: an emerging tool for image-guided radiotherapy. Am J Clin Oncol 2007; 30: pp. 617-623.
10. Suh J.H., Gardner J.M., Kee K.H., et. al.: Calcifications in prostate and ejaculatory system: a study on 298 consecutive whole mount sections of prostate from radical prostatectomy or cystoprostatectomy specimens. Ann Diagn Pathol 2008; 12: pp. 165-170.
11. Kupelian P.A., Langen K.M., Willoughby T.R., et. al.: Image-guided radiotherapy for localized prostate cancer: treating a moving target. Semin Radiat Oncol 2008; 18: pp. 58-66.
12. Zeng G.G., McGowan T.S., Larsen T.M., et. al.: Calcifications are potential surrogates for prostate localization in image-guided radiotherapy. Int J Radiat Oncol Biol Phys 2008; 72: pp. 963-966.