
Rationale and Objectives
The long-term prospects for patients with peripheral-arterial-occlusive disease (PAOD) must be considered in the context of coexistent generalized atherosclerosis. We sought to determine the added clinical information of noninvasive magnetic resonance imaging (MRI) for detecting asymptomatic atherosclerotic disease in patients already at high risk.
Materials and Methods
Eighty-four patients (64 men, mean age 66.2 ± 10.0 years, range 34–84 years) with suspected or known PAOD were examined using a comprehensive cardiovascular MRI protocol. Two experienced observers reviewed all MRIs for the presence of “relevant findings,” which were defined as pathology requiring immediate therapy or mid-term follow-up.
Results
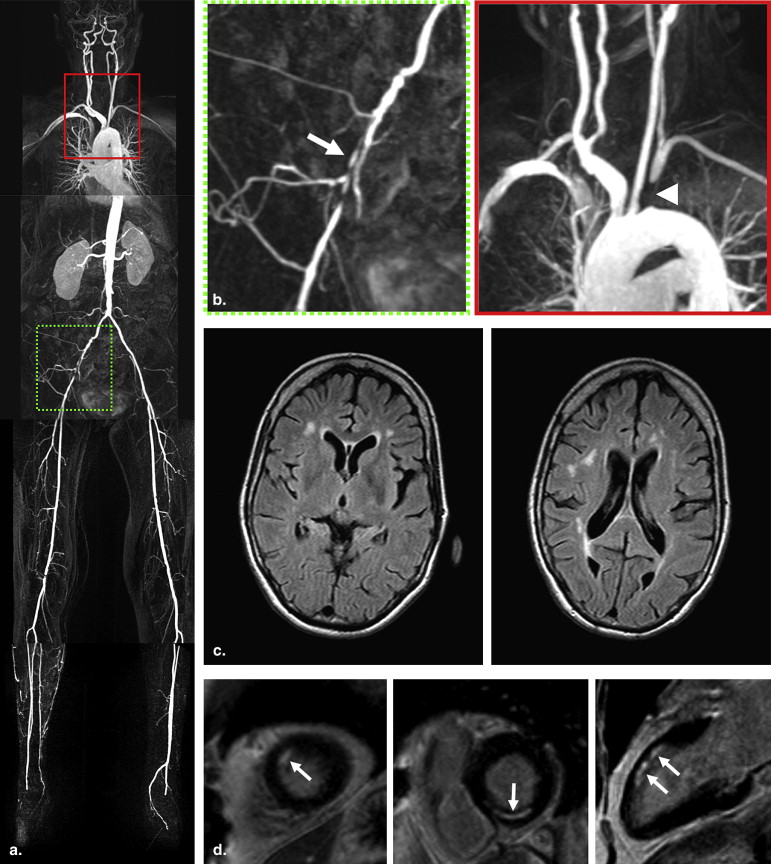
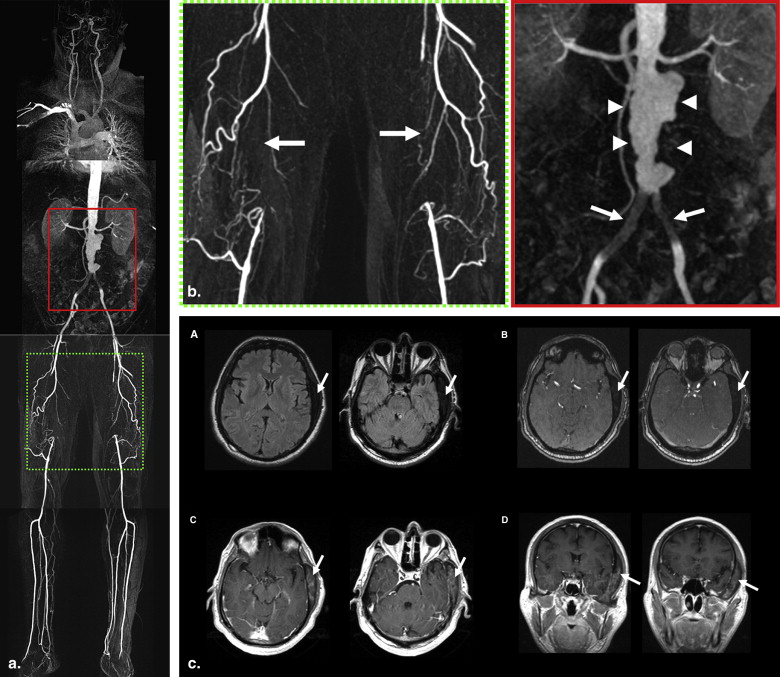
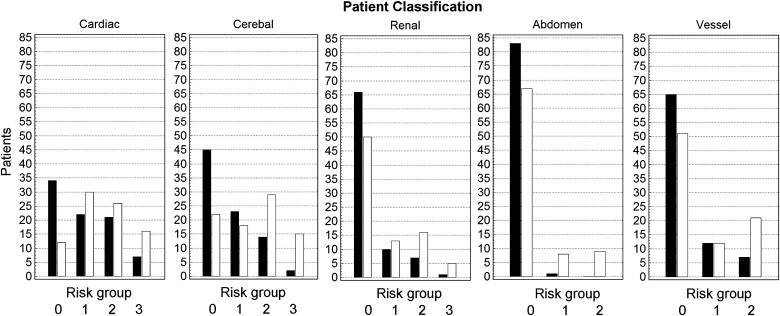
Assessment of cardiac structures and function in 84 study patients yielded new pathology in 40 (48%) patients, whereas cerebral imaging revealed new findings in 45 (54%) patients. Previously unsuspected vascular findings were evident in 46 (55%) patients. Using the information from the MRIs, in 54 (64%) of patients mid-term follow-up was required, whereas in 7 (8%) patients a change of therapy or immediate treatment was necessary.
Conclusion
Whole-body cardiovascular MRI is able to detect symptomatic and unsuspected findings in patients with PAOD. This technique was able to detect several vascular abnormalities that necessitated immediate medical attention and intervention in patients already identified as high-risk patients and, therefore, may show an increasing impact to determine individual therapeutic and follow-up concepts.
Cardiovascular disease (CVD) is a leading cause of death worldwide and accounts for almost 17 million deaths annually. Nearly 80% of these deaths occur in developed countries, mainly as a result of the aging of the population . Ideally, in a patient with systemic atherosclerotic disease, besides management and medical treatment of atherosclerotic risk factors, all major sites of atherosclerotic manifestation should be addressed in order to improve clinical outcomes and quality of life.
A high absolute cardiovascular risk, as defined, for example, by the SCORE (systematic coronary risk evaluation) mortality risk table , requires drastic lifestyle changes and medical treatment of atherosclerotic risk factors, whereas patients at low to moderate risk are mainly advised to adhere to lifestyle modifications. Noninvasive vascular imaging may be used for identifying patients initially considered to have a low vascular risk but, after detecting asymptomatic atherosclerotic disease, to reconsider these patients as high vascular risk . Patients with a (recent) clinical manifestation of an atherosclerotic disease are already classified as high risk; however, noninvasive vascular imaging may be useful in detecting vascular abnormalities that necessitate immediate medical attention (eg, aortic aneurysms, carotid artery stenosis). Because of the generalized nature of atherosclerosis, the prevalence of asymptomatic vascular diseases is high in these patients . In those patients with significant coexisting disease, myocardial revascularization therapies may improve myocardial perfusion and reduce the risk of myocardial infarction and heart failure; treatment of carotid stenoses permits survival with reduced incidence of stroke; renal artery angioplasty reduces the incidence of renal insufficiency and the need for dialysis and transplantation; and, finally, treatment of lower extremity arterial occlusive disease may improve quality of life and functional status, facilitate wound healing, and decrease amputation rates. In patients who are scheduled for surgical interventions, undetected accompanying atherosclerotic disease may largely affect the surgical outcome or dramatically increase perioperative complication rates .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Patient Population
Get Radiology Tree app to read full this article<
MRI Protocol
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Interpretation of Images
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Patient Classification and Categorization of MRI Findings
Get Radiology Tree app to read full this article<
Table 1
Classification of Disease Categories Based on Patients’ Chart and Vascular History
Disease category Inclusion diagnosis Vascular history ∗ Peripheral arterial disease Intermittent claudication, rest pain, gangrene, ulcers, resting ABPI ≤0.90 Arterial operation; PTA leg; amputation leg Aneurysm of abdominal aorta Distal aortic anteroposterior diameter >3.0 cm or distal/proximal ratio ≥1.5 cm Surgery for aneurysm Cerebrovascular disease Cerebral ischemia, transient ischemic attack, amaurosis fugax, minor ischemic stroke, retinal infarction, or asymptomatic carotid artery stenosis with diameter reduction ≥30% Transient ischemic attack; stroke Coronary heart disease Myocardial infarction—at least 2 of the following criteria:
1. Chest pain for at least 20 minutes not disappearing after administration of nitrates
2. ST elevation >1 mm in 2 following leads or a left bundle branch block on the ECG
3. CK elevation of at least 2 times the normal value of CK and an MB fraction >5% of the total CK
Angina pectoris: chest pain with or without documented ischemia on the ECG and with documented stenosis on the angiography Myocardial infarction; angina pectoris
CABG or PTCA Arterial hypertension Systolic BP ≥140 mm Hg, diastolic BP ≥90 mm Hg, or antihypertensive agent use Hyperlipidemia Total cholesterol ≥5.0 mmol/L, LDL cholesterol ≥3.0 mmol/L, or lipid-lowering drug use Diabetes mellitus type 1 and 2 Fasting glucose ≥7.0 mmol/L, nonfasting glucose ≥11.0 mmol/L, or oral antidiabetic drug or insulin use Adipositas BMI ≥ 30 kg/m 2 Smoking History of ≥ 5 py
ECG, electrocardiogram; CK, creatinine kinase; MB, myocardial band; CABG, coronary artery bypass graft; PTCA, percutaneous transluminal coronary angioplasty; PTA, percutaneous transluminal angioplasty; ABPI, ankle brachial pressure index; BP, blood pressure; LDL, low-density lipoprotein; py, pack-years.
Get Radiology Tree app to read full this article<
Table 2
Demographic and Clinical Characteristics of the 84 Study Patients
Female sex: no. (%) 20 (24) Age (y) Mean ± SD 66 ± 10 Range 34–84 Peripheral arterial occlusive disease (no.) (%) Fontaine stage IIb 75 (89) Fontaine stage III 1 (1) Fontaine stage IV 8 (10) Cerebrovascular disease (no.) (%) 62 (74) Coronary heart disease (no.) (%) 72 (86) Arterial hypertension (no.) (%) 63 (75) Hyperlipidemia (no.) (%) 44 (52) Diabetes mellitus type 1 and 2 (no.) (%) 23 (27) Adipositas (no.) (%) 20 (24) Current or prior cigarette smoking (no.) (%) 53 (63) Family history of cardiovascular events (MI, stroke) (no.) (%) ∗ 7 (8) Accumulation of cardiovascular risk factors per patient (no.) (%) † No risk factors 3 (4) One risk factor 16 (19) Two risk factors 23 (27) Three risk factors 24 (29) Four risk factors 13 (15) Five risk factors 4 (5) Six risk factors 1 (1) 10-year predicted risk of developing manifest coronary heart disease according to Framingham risk index Mean ± SD 24.9 ± 14.0 Relative risk compared to age-matched control group according to Mean ± SD 2.6 ± 1.4
MI, myocardial infarction; PAOD, peripheral arterial occlusive disease; SD, standard deviation.
Definition of categories according to Table 1 .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Calculation of Framingham Risk Index
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Additional MRI Findings
Severity 0 1 2 3 Cardiac No (additional) pathology Discrete reduction of LV function (EF 45%–54%) or normal EF with segmental wall motion abnormalities or low-grade pathology (eg, mild valvular pathology, unspecific DE, discrete subendocardial DE) Moderate reduction of LV function (EF 35%–44%) or medium-grade pathology (eg, subendocardial DE) Severe reduction of left ventricular function (EF <35%) or high-grade pathology (eg, high-grade valvular pathology, transmural DE, LV aneurysm, pericardial effusion) Cerebral No (additional) pathology Hemodynamically nonsignificant CVD or low-grade pathology (eg, extensive microvascular disease) Hemodynamically significant CVD or medium-grade pathology (eg, lacunary ischemia, small cerebral infarction/apoplexy) Bilateral hemodynamically significant CVD or high-grade pathology (eg, large cerebral infarction, acute ischemia, cerebral tumor) Renal No (additional) pathology Hemodynamically nonsignificant RAS or low-grade pathology (eg, multicystic kidney disease) Hemodynamically significant RAS or medium-grade pathology (eg, hypoplastic kidney) Bilateral hemodynamically significant RAS or high-grade pathology (eg, renal tumor) Abdominal No (additional) pathology Hemodynamically non significant stenosis of celiac trunk/SMA/IMA or low-grade pathology (eg, Hx of abdominal angina) Hemodynamically significant stenosis of celiac trunk/SMA/IMA or high-grade pathology (eg, Hx of bowel ischemia) NA Peripheral No (additional) pathology/stenosis to primary Dx Hemodynamically non significant stenosis or moderate AAA (≤55 mm in diameter) Hemodynamically significant stenosis or large AAA (>55 mm in diameter or expansion >1 cm/year) NA
CVD, cerebrovascular disease; DE, delayed enhancement; Dx, diagnosis; EF, ejection fraction; Hx, history; IMA, inferior mesenteric artery; LV, left ventricle; NA, not applicable; RAS, renal artery stenosis; SMA, superior mesenteric artery.
Modified from .
Get Radiology Tree app to read full this article<
Patient Follow-up
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Cardiac Pathology
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Cerebral and Cerebrovascular Pathology
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Renal, Abdominal, and Peripheral Vascular Pathology
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Detected High-grade Lesions
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Limitations
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Smith S.C., Jackson R., Pearson T.A., et. al.: Principles for national and regional guidelines on cardiovascular disease prevention: a scientific statement from the World Heart and Stroke Forum. Circulation 2004; 109: pp. 3112-3121.
2. Conroy R.M., Pyorala K., Fitzgerald A.P., et. al.: Estimation of ten-year risk of fatal cardiovascular disease in Europe: the SCORE project. Eur Heart J 2003; 24: pp. 987-1003.
3. de Backer G., Ambrosioni E., Borch-Johnsen K., et. al.: European guidelines on cardiovascular disease prevention in clinical practice: third joint task force of European and other societies on cardiovascular disease prevention in clinical practice (constituted by representatives of eight societies and by invited experts). Eur J Cardiovasc Prev Rehabil 2003; 10: pp. S1-S10.
4. de Backer G., Ambrosioni E., Borch-Johnsen K., et. al.: (2003) European guidelines on cardiovascular disease prevention in clinical practice. Third joint task force of European and other societies on cardiovascular disease prevention in clinical practice. Eur Heart J 2003; 24: pp. 1601-1610.
5. Kurvers H.A., van der G.Y., Blankensteijn J.D., et. al.: Screening for asymptomatic internal carotid artery stenosis and aneurysm of the abdominal aorta: comparing the yield between patients with manifest atherosclerosis and patients with risk factors for atherosclerosis only. J Vasc Surg 2003; 37: pp. 1226-1233.
6. Faggioli G.L., Curl G.R., Ricotta J.J.: The role of carotid screening before coronary artery bypass. J Vasc Surg 1990; 12: pp. 724-731.
7. Schwartz L.B., Bridgman A.H., Kieffer R.W., et. al.: Asymptomatic carotid artery stenosis and stroke in patients undergoing cardiopulmonary bypass. J Vasc Surg 1995; 21: pp. 146-153.
8. Goessens B.M., Visseren F.L., Algra A., et. al.: Screening for asymptomatic cardiovascular disease with noninvasive imaging in patients at high-risk and low-risk according to the European guidelines on cardiovascular disease prevention: the SMART study. J Vasc Surg 2006; 43: pp. 525-532.
9. Alexander J.A., Sheppard S., Davis P.C., et. al.: Adult cerebrovascular disease: role of modified rapid fluid-attenuated inversion-recovery sequences. Am J Neuroradiol 1996; 17: pp. 1507-1513.
10. Kim R.J., Wu E., Rafael A., et. al.: The use of contrast-enhanced magnetic resonance imaging to identify reversible myocardial dysfunction. N Engl J Med 2000; 343: pp. 1445-1453.
11. Fenchel M., Scheule A.M., Stauder N.I., et. al.: Atherosclerotic disease: whole-body cardiovascular imaging with MR system with 32 receiver channels and total-body surface coil technology—initial clinical results. Radiology 2006; 238: pp. 280-291.
12. Cerqueira M.D., Weissman N.J., Dilsizian V., et. al.: (2002) Standardized myocardial segmentation and nomenclature for tomographic imaging of the heart: a statement for healthcare professionals from the cardiac imaging committee of the council on clinical cardiology of the American Heart Association. Circulation 2002; 105: pp. 539-542.
13. Wilson P.W.F., D’Agostino R.B., Levy D., et. al.: Prediction of coronary heart disease using risk factor categories. Circulation 1998; 97: pp. 1837-1847.
14. Fenchel M., Jost D., Kramer U., et. al.: Cardiovascular whole-body MR imaging in patients with symptomatic peripheral arterial occlusive disease. Fortschr Roentgenstr 2006; 178: pp. 491-499.
15. Barth A., Arnold M., Mattle H.P., et. al.: Contrast-enhanced 3-D MRA in decision making for carotid endarterectomy: a 6-year experience. Cerebrovasc Dis 2006; 21: pp. 393-400.
16. Hansen T., Ahlstrom H., Wikstrom J., et. al.: A total atherosclerotic score for whole-body MRA and its relation to traditional cardiovascular risk factors. Eur Radiol 2008; 18: pp. 1174-1180.
17. Mistry S., Ives N., Harding J., et. al.: Angioplasty and Stent for Renal Artery Lesions (ASTRAL trial): rationale, methods and results so far. J Hum Hypertens 2007; 21: pp. 511-515.
18. Eagle K.A., Guyton R.A., Davidoff R., et. al.: ACC/AHA guidelines for coronary artery bypass graft surgery: executive summary and recommendations: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to revise the 1991 guidelines for coronary artery bypass graft surgery). Circulation 1999; 100: pp. 1464-1480.
19. Tunio A.M., Hingorani A., Ascher E.: The impact of an occluded internal carotid artery on the mortality and morbidity of patients undergoing coronary artery bypass grafting. Am J Surg 1999; 178: pp. 201-205.
20. Da Silva A., Widmer L.K., Ziegler H.W., et. al.: The Basle longitudinal study: report on the relation of initial glucose level to baseline ECG abnormalities, peripheral artery disease, and subsequent mortality. J Chron Dis 1979; 32: pp. 797-803.
21. Wolff T., Guirguis-Blake J., Miller T., et. al.: Screening for carotid artery stenosis: an update of the evidence for the U.S. Preventive Services Task Force. Ann Intern Med 2007; 147: pp. 860-870.
22. Liapis C.D., Bell P.R., Mikhailidis D., et. al.: ESVS guidelines. Invasive treatment for carotid stenosis: indications, techniques. Eur J Vasc Endovasc Surg 2009; 37: pp. 1-19.
23. Kazmers A., Cerquiera M.D., Zierler M.E.: Perioperative and late outcome in patients with left ventricular ejection fraction of 35% or less who require major vascular surgery. J Vasc Surg 1988; 8: pp. 307-315.
24. Wagner A., Mahrholdt H., Holly T.A., et. al.: Contrast-enhanced MRI and routine single photon emission computed tomography (SPECT) perfusion imaging for detection of subendocardial myocardial infarcts: an imaging study. Lancet 2003; 361: pp. 374-379.
25. Criqui M.H., Langer R.D., Fronek A., et. al.: Mortality over a period of 10 years in patients with peripheral arterial disease. N Engl J Med 1992; 326: pp. 381-386.
26. Nagel E., Klein C., Paetsch I., et. al.: Magnetic resonance perfusion measurements for the noninvasive detection of coronary artery disease. Circulation 2003; 108: pp. 432-437.
27. Al-Saadi N., Nagel E., Gross M., et. al.: Noninvasive detection of myocardial ischemia from perfusion reserve based on cardiovascular magnetic resonance. Circulation 2000; 101: pp. 1379-1383.
28. Miller S., Helber U., Brechtel K., et. al.: MR imaging at rest early after myocardial infarction: detection of preserved function in regions with evidence for ischemic injury and non-transmural myocardial infarction. Eur Radiol 2003; 13: pp. 498-506.
29. Lawson M.A., Johnson L.L., Coghlan L., et. al.: Correlation of thallium uptake with left ventricular wall thickness by cine magnetic resonance imaging in patients with acute and healed myocardial infarcts. Am J Cardiol 1997; 80: pp. 434-441.
30. Kramer H., Michaely H.J., Reiser M.F., et. al.: Peripheral magnetic resonance angiography at 3.0 T. Top Magn Reson Imaging 2007; 18: pp. 135-138.
31. Nael K., Fenchel M., Krishnam M., et. al.: High-spatial-resolution whole-body MR angiography with high-acceleration parallel acquisition and 32-channel 3.0-T unit: initial experience. Radiology 2007; 242: pp. 865-872.
32. von Kemp K., van den Brande P., Peterson T., et. al.: Screening for concomitant diseases in peripheral vascular patients. Results of a systematic approach. Int Angiol 1997; 16: pp. 114-122.