
Rationale and Objectives
Scanning parameters used in multislice computed tomographic (MSCT) coronary angiography should be adapted to patients’ heart rates. The aim of this study was to evaluate the rate of success of a software-assisted scan simulation to determine optimal gantry rotation time prior to MSCT coronary angiography.
Materials and Methods
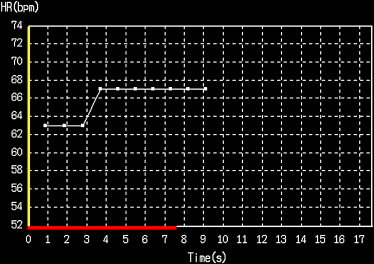
Data from 218 64-slice MSCT coronary angiographic studies were retrospectively analyzed. Prior to the MSCT examination, a scan had been simulated by giving a breath-hold command, after which a software program recorded the patient’s heart rate from an electrocardiogram over the expected scanning time and predicted optimal scanning parameters. The success rate in predicting optimal parameters for the subsequent MSCT examination and the resulting acquisition window width were analyzed.
Results
There was a wide range of heart rates among the patients. The mean intraindividual variation during scan simulation and examination was 4.8 beats/min. Optimal scan parameters were selected in 179 of 218 cases (82%). The median acquisition window width achieved in this group was 174 ms (range, 100–200), compared with 192 ms (range, 149–225) in cases in which suboptimal settings were selected ( P < .001). Correct prediction occurred significantly more often in patients with low heart rates (<66 beats/min) than in those with higher heart rates (≥66 beats/min) (93% vs 66%; P < .001).
Conclusions
The software-assisted scan simulation was a fast and simple procedure that allowed the selection of optimal computed tomographic parameters in >80% of patients. The procedure may be a useful adjunct to avoid unwanted synchronicity of gantry rotation and heart cycle and optimize temporal resolution in MSCT coronary angiography.
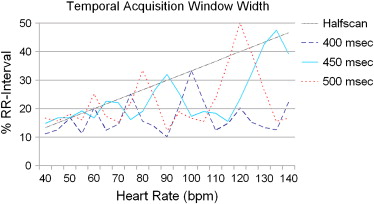
Coronary angiography using noninvasive techniques might provide a reliable basis for clinical decision making in patients with suspected coronary artery disease ( ). However, noninvasive coronary imaging requires high temporal and spatial resolution of the coronary arteries ( ). The temporal resolution achieved with the standard half-scan reconstruction method of computed tomography may be inadequate to avoid significant motion artifacts, especially in patients with high heart rates and thus faster movement of the coronary arteries. A few studies have shown that multisegment reconstruction is a useful technique to increase temporal resolution and thus reduce motion artifacts in multislice computed tomographic (MSCT) coronary angiography, particularly in patients with higher heart rates ( ). However, this technique requires a computed tomographic (CT) scanner capable of varying the gantry rotation time to avoid synchrony of gantry rotation and the cardiac cycle at certain heart rates. To maximize temporal resolution, the optimal gantry rotation time, depending on the patient’s heart rate, must be chosen prior to examination ( ). This may be achieved by measuring heart rate during free breathing with an electrocardiographic (ECG) monitor prior to the coronary CT examination. However, there are possible sources of inaccuracy in this approach: normal variation in heart rate is not taken into consideration, and the physiologic effects of apnea are lacking. Heart rate has been shown to change between free breathing and apnea, even during the short period of time required for cardiac CT imaging ( ). A further source of variability may be the results of contrast agent application, which represents a volume load and may have direct effects on myocardial contractility ( ).
Some scanners offer a software-based approach to adapting gantry rotation time and pitch to patients’ heart rates on the basis of measurement of the heart rate in apnea during a simulated scan period prior to examination. We aimed to assess the rate of success of the technique in the selection of optimal scanning parameters, defined as the combination of settings yielding the highest temporal resolution, and to quantify the temporal acquisition window width achieved in a clinical setting.
Materials and methods
Patients
Get Radiology Tree app to read full this article<
Scan Simulation
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Categories of Settings According to Heart Rate and Number of Patients Assigned to Each Category During the Scan Simulation and During the Examination
Number of Patients (%) Heart Rate (beats/min) Gantry Rotation Time (seconds) Pitch Reconstruction Mode Scan Simulation Examination 30–50 0.4 0.2–0.223 Half scan 4 (2%) 11 (5%) 51–72 0.4 0.225 Multisegment 185 (85%) 153 (70%) 73–79 0.45 0.253 Multisegment 19 (9%) 31 (14%) 80–92 0.4 0.225 Multisegment 7 (3%) 21 (10%) 93–99 0.5 0.281 Multisegment 2 (1%) 1 (0.5%) 100–110 0.45 0.253 Multisegment 1 (0.5%) 1 (0.5%)
Get Radiology Tree app to read full this article<
MSCT Coronary Angiography
Get Radiology Tree app to read full this article<
Statistical analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Median Temporal Acquisition Window Width According to Correct or Incorrect Prediction of Optimal Settings
Median Temporal Acquisition Window Width (ms) Heart Rate (beats/min) Correct Prediction Incorrect Prediction Overall ≥66 ( n = 89) 157 ⁎ 189 ⁎ 163 ‡ <66 ( n = 129) 178 † 200 † 178 ‡
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Advantages and Limitations of the Technique
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Limitations of the Study
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
References
1. Hoffmann H., Dubel H.P., Laube H., Hamm B., Dewey M.: Triage of patients with suspected coronary artery disease using multislice computed tomography. Acad Radiol 2007; 14: pp. 901-909.
2. Ropers U., Ropers D., Pflederer T., et. al.: Influence of heart rate on the diagnostic accuracy of dual-source computed tomography coronary angiography. J Am Coll Cardiol 2007; 50: pp. 2393-2398.
3. Dewey M., Hamm B.: CT coronary angiography: examination technique, clinical results, and outlook on future developments. Rofo 2007; 179: pp. 246-260.
4. Lembcke A., Rogalla P., Mews J., et. al.: Imaging of the coronary arteries by means of multislice helical CT: optimization of image quality with multisegmental reconstruction and variable gantry rotation time. Rofo 2003; 175: pp. 780-785.
5. Hoffmann M.H., Shi H., Manzke R., et. al.: Noninvasive coronary angiography with 16-detector row CT: effect of heart rate. Radiology 2005; 234: pp. 86-97.
6. Dewey M., Laule M., Krug L., et. al.: Multisegment and halfscan reconstruction of 16-slice computed tomography for detection of coronary artery stenoses. Invest Radiol 2004; 39: pp. 223-229.
7. Dewey M., Teige F., Laule M., Hamm B.: Influence of heart rate on diagnostic accuracy and image quality of 16-slice CT coronary angiography: comparison of multisegment and halfscan reconstruction approaches. Eur Radiol 2007; 17: pp. 2829-2837.
8. Greuter M.J., Flohr T., van Ooijen P.M., Oudkerk M.: A model for temporal resolution of multidetector computed tomography of coronary arteries in relation to rotation time, heart rate and reconstruction algorithm. Eur Radiol 2007; 17: pp. 784-812.
9. Zhang J., Fletcher J.G., Scott Harmsen W., et. al.: Analysis of heart rate and heart rate variation during cardiac CT examinations. Acad Radiol 2008; 15: pp. 40-48.
10. Chuck L.H., Refsum H., Rouleau J.L., Mathey D., Sievers R.E., Parmley W.W.: Direct pharmacologic and osmolal effects of contrast media on the mechanics of heart muscle isolated from cats. Am Heart J 1984; 108: pp. 97-104.
11. Dawson P.: Cardiovascular effects of contrast agents. Am J Cardiol 1989; 64: pp. 2E-9E.
12. Roriz R., de Gevigney G., Finet G., et. al.: Comparison of iodixanol (Visipaque) and ioxaglate (Hexabrix) in coronary angiography and ventriculography: a double-blind randomized study. J Radiol 1999; 80: pp. 727-732.
13. Vik-Mo H., Danielsen R., Skinningsrud K., Haider T., Bjorkhaug A.: Cardiovascular and electrocardiographic effects of iopentol in left ventricular angiography. Eur Radiol 1997; 7: pp. S156-S161.
14. Blobel J., Baartman H., Rogalla P., Mews J., Lembcke A.: Spatial and temporal resolution with 16-slice computed tomography for cardiac imaging. Rofo 2003; 175: pp. 1264-1271.
15. Leber A.W., Johnson T., Becker A., et. al.: Diagnostic accuracy of dual-source multi-slice CT-coronary angiography in patients with an intermediate pretest likelihood for coronary artery disease. Eur Heart J 2007; 28: pp. 2354-2360.
16. Song S.H., Lee W.K., Chung Y.A., Hong S.K.: Mechanism of apneic bradycardia in man. J Appl Physiol 1969; 27: pp. 323-327.