
Rationale and Objectives
Patient-centered outcome measures have become an essential focus in research methodology in recent years. This may be particularly challenging in imaging research at the technology assessment level to incorporate patient-centeredness. A primary issue in this field is designing a reference standard that is applicable to the entire study population.
Materials and Methods
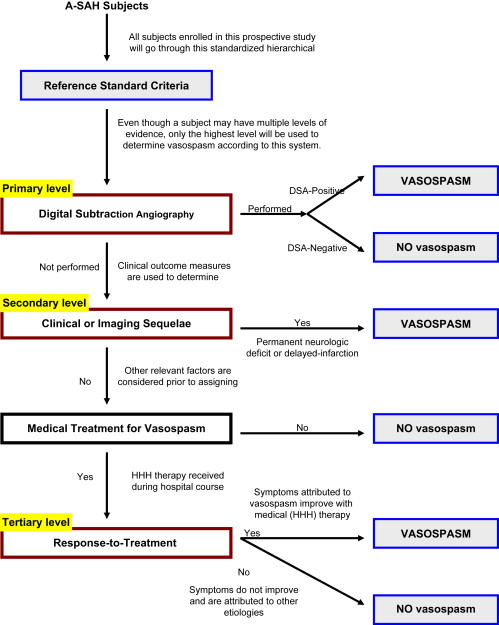
This important element is necessary for translation of findings into clinical practice. In our work, computed tomographic perfusion imaging is being evaluated as a new technology used in aneurysmal subarachnoid hemorrhage patients to detect cerebral vasospasm. We have developed a new reference standard employing a multistage hierarchical design incorporating both clinical and imaging criteria to determine a diagnosis of vasospasm.
Results
A flowchart of the reference standard levels is provided for illustration. The limitations and potential biases that may occur using this reference standard are discussed.
Conclusions
This reference standard will be applicable to the entire study population, including those with and without symptoms or further imaging with digital subtraction angiography.
In the past several years, there has been growing public interest in the management of health care, resource allocation, and improving patient outcomes. Patient involvement in health care issues has become a primary initiative by the consumer and government policy makers. It is our interest to incorporate patient-centeredness into research methodology using outcome measures. However, it may be challenging particularly in imaging research at the technology assessment level to incorporate patient-centeredness into research methodology. Littenberg describes incorporating the overall medical, psychologic, and financial effects of the technology into assessing patient outcomes. This includes the unintended side effects and long-term morbidity and mortality. The selection of an appropriate reference standard that is representative of patient outcomes from a patients’ perspective is complex. The primary obstacle to overcome is to design a reference standard that is applicable to the entire population that the imaging study is intended for use in clinical practice. Analyses performed on a subgroup of the population due to limitations with the reference standard, such as only symptomatic patients receive the reference standard test, may yield important findings that are not translatable to the clinical population. This limitation is not always recognized when applying the literature in clinical practice for determining management and treatment decisions.
In our work, computed tomographic perfusion (CTP) is being evaluated as a new technology used in aneurysmal subarachnoid hemorrhage (A-SAH) patients to detect cerebral vasospasm. In the clinical care setting, CTP is intended for use on all patients with A-SAH, including patients with and without symptoms. It then becomes important to implement a reference standard in the research methodology that is applicable to the entire target population, including those with and without symptoms and those who will not have additional imaging performed. We have specifically developed a new reference standard to address these limitations using a multistage hierarchical design incorporating both clinical and imaging criteria for determination of vasospasm.
Patient population
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Reference standard design
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Littenberg B.: A practice guideline revisited: screening for hypertension. Ann Intern Med 1995; 122: 937–199
2. Ingal I.T.J., Whisnant J.P.: Epidemiology of subarachnoid hemorrhage.Yanagihara T.Pepegras D.C.Atkinson J.L.D.Subarachnoid hemorrhage: medical and surgical management.1998.Marcel DekkerNew York, NY:pp. 194-206.
3. Hop J.W., Rinkel G.J., Algra A., et. al.: Case fatality rates and functional outcome after subarachnoid hemorrhage: a systematic review. Stroke 1997; 28: pp. 660-664.
4. Biller J., Godersky J.C., Adams H.P.: Management of aneurysmal subarachnoid hemorrhage. Stroke 1988; 19: pp. 1300-1305.
5. Baldwin M.E., Macdonald R.L., Huo D.: Early vasospasm on admission angiography in patients with aneurysmal subarachnoid hemorrhage is a predictor for in hospital complications and poor outcome. Stroke 2004; 35: pp. 2506-2511.
6. Earnst F., Forbes G., Sandok B.A., et. al.: Complications of diagnostic cerebral angiography: prospective assessment of risk. Am J Roentgenol 1984; 142: pp. 247-253.
7. Pryor J.C., Setton A., Nelson P.K., et. al.: Complications of diagnostic cerebral angiography and tips on avoidance. Neuroimaging Clin N Am 1996; 6: pp. 751-758.
8. Macdonald L.R., Weir B.: Medical aspects of vasospasm. Cerebral vasospasm.2001.Academic PressSan Diego 353–458
9. Powers W.J., Grubb R.L., Baker R.P., et. al.: Regional cerebral blood flow and metabolism in reversible ischemia due to vasospasm. J Neurosurg 1985; 62: pp. 539-546.
10. Kawamura S., Sayama I., Yasui N., et. al.: Sequential changes in cerebral blood flow and metabolism in patients with subarachnoid hemorrhage. Acta Neurochir 1992; 114: pp. 12-15.
11. Soucy J.P., McNamara D., Mohr G., et. al.: Evaluation of vasospasm secondary to subarachnoid hemorrhage with technetium-99m-hexamethyl-propyleneamine oxime (HM-PAO) tomoscintigraphy. J Nucl Med 1990; 31: pp. 972-976.
12. Rordorf G., Koroshetz W.J., Copen W.A., et. al.: Diffusion- and perfusion-weighted imaging in vasospasm after subarachnoid hemorrhage. Stroke 1999; 30: pp. 599-614.
13. Nabavi D.G., LeBlanc L.M., Baxter B., et. al.: Monitoring cerebral perfusion after subarachnoid hemorrhage using CT. Neuroradiology 2001; 43: pp. 7-16.
14. Knuckey N.W., Fox R.A., Surveyor I., et. al.: Early cerebral blood flow and computerized tomography in predicting ischemia after cerebral aneurysm rupture. J Neurosurg 1985; 62: pp. 850-855.
15. Geraud G., Tremoulet M., Guell A., et. al.: The prognostic value of non-invasive CBF measurements in subarachnoid hemorrhage. Stroke 1984; 15: pp. 301-305.
16. Ferguson G.G., Harper A.M., Fitch W., et. al.: Cerebral blood flow measurements after spontaneous subarachnoid hemorrhage. Eur Neurol 1972; 8: pp. 15-22.
17. Wardlaw J.M., Offin R., Teasdale G.M., et. al.: Is routine transcranial Doppler ultrasound monitoring useful in the management of subarachnoid hemorrhage?. J Neurosurg 1998; 88: pp. 272-276.
18. Carpenter D.A., Grubb R.L., Tempel L.W., et. al.: Cerebral oxygen metabolism after aneurysmal subarachnoid hemorrhage. J Cereb Blood Flow Metab 1991; 11: pp. 837-844.
19. Yundt K.D., Grubb R.L., Diringer M.N., et. al.: Autoregulatory vasodilation of parenchymal vessels is impaired during cerebral vasospasm. J Cereb Blood Flow Metab 1998; 18: pp. 419-424.
20. Kaid M.S., Souter M.J., Treggiari M.M., et. al.: Accuracy of transcranial Doppler ultrasonography and single photon emission computed tomography in the diagnosis of angiographically demonstrated cerebral vasospasm. J Neurosurg 2009; 110: pp. 67-72.
21. Wintermark M., Ko N.U., Smith W., et. al.: Vasospasm after subarachnoid hemorrhage: utility of perfusion CT and CT angiography on diagnosis and management. Am J Neuroradiol 2006; 27: pp. 26-34.
22. Mani R.L., Eisenberg R.L., McDonald E.J., et. al.: Complications of catheter cerebral arteriography: analysis of 5,000 procedures. I. Criteria and incidence. AJR Am J Roentgenol 1978; 131: pp. 861-865.