
Rationale and Objectives
The American Institute of Ultrasound in Medicine (AIUM) recommends that all providers performing ultrasound-guided invasive procedures be competent in a core set of guidance skills common to all ultrasound-guided procedures, including in-plane and out-of-plane needle guidance and needle imaging optimization techniques such as probe translation, rotation, and heel-toe standoff. To allow for the practice and assessment of these core skills, we have created a novel task trainer and set of targeting tasks, and sought to obtain validity evidence in the content and response process domains for this training and assessment system according to the Standards for Educational and Psychological Testing.
Materials and Methods
We have constructed an ultrasound-guided invasive procedure training system and five targeting tasks that focused on the needle guidance skills outlined by the AIUM. All tasks were performed by obstetrics and gynecology or maternal-fetal medicine physicians with and without experience in ultrasound-guided invasive procedures during a series of simulation workshops. All participants completed a survey regarding the trainer’s and the tasks’ usefulness in the training of inexperienced physicians.
Results
The physicians who completed the tasks had favorable views of task trainer and curriculum. The targeting curriculum was felt to allow practice of all of the core guidance skills outlined by the AIUM. The average response provided for all of the tasks was 4.0 or greater, with half of the items having an average response of 4.5 or higher.
Conclusions
We have constructed a task trainer that incorporates all of the core skills outlined by the AIUM. All five tasks received very favorable reviews from both experienced and inexperienced providers. Taken together, our findings suggest they have strong content and response process validity evidence.
Introduction
With the dramatic improvements in ultrasound technology seen in recent years, many invasive procedures in a variety of medical fields that were performed blindly are now being performed with the aid of ultrasound guidance. Examples include paracentesis, central line placement, and amniocentesis, among numerous others. With the introduction of resident duty hour restrictions and the replacement of invasive procedures with noninvasive tests, it is now difficult for trainees to gain enough real-life experience during residency or fellowship to independently perform these procedures after graduation. The classic “see one, do one, teach one” training paradigm has become unsustainable.
As an example, in obstetrics and gynecology (OB/GYN), studies have demonstrated that between 50 and 100 procedures are required before a provider can become competent in amniocentesis . In chorionic villus sampling (CVS), a single study demonstrated that 100 procedures were required to obtain competence . These numbers of procedures are virtually impossible to obtain in a 4-year OB/GYN residency and remain difficult to achieve with an additional 3-year maternal-fetal medicine (MFM) fellowship. The same difficulties are encountered in interventional radiology. In 2013, the Society of Interventional Radiology outlined the minimum number of procedures required for graduation , including (1) 100 percutaneous vascular punctures, (2) 200 selective vascular catheterizations, (3) 50 vascular angioplasties, (4) 25 vascular stent placements, (5) 50 embolization procedures, and (6) 50 image-guided nonvascular procedures. These are very ambitious numbers for the combined 4 years of residency and 1 year of fellowship required for certification in interventional radiology.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Methods
Task Trainer Construction
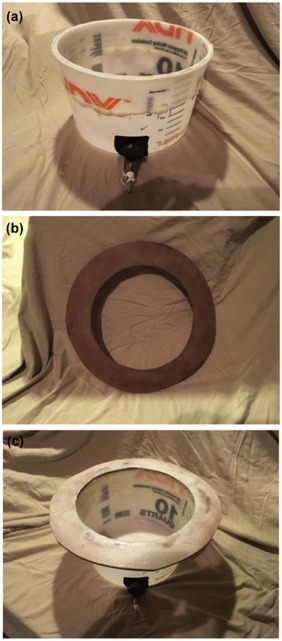
Ballistic Gelatin Simulated Body Walls
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Container
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
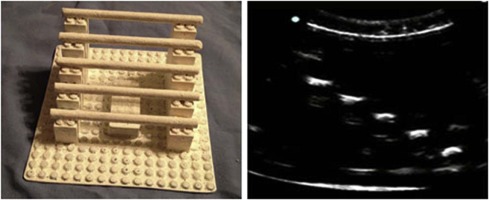
Dowel Targeting Model
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
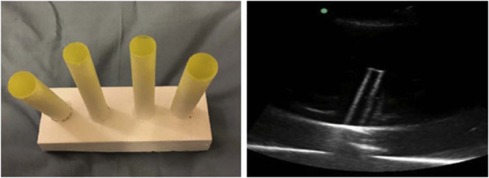
Straw Targeting Model
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
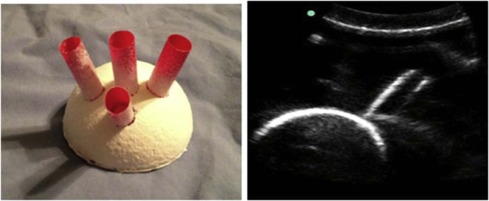
Ball Targeting Model
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Heel-toe Targeting Model
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Targeting Tasks
Get Radiology Tree app to read full this article<
In-plane Dowel Task
Get Radiology Tree app to read full this article<
Out-of-plane Dowel Task
Get Radiology Tree app to read full this article<
Straw Task
Get Radiology Tree app to read full this article<
Ball Task
Get Radiology Tree app to read full this article<
Heel-toe Task
Get Radiology Tree app to read full this article<
Assessment of Trainer Response Process
Get Radiology Tree app to read full this article<
TABLE 1
Provider Survey Results
Survey Item Inexperienced Experienced 1. The in-plane dowel task simulated a technical challenge encountered in clinical practice. 4.4 ± 0.6 4.4 ± 0.6 Strongly Disagree (1) Disagree (2) Neutral (3) Agree (4) Strongly Agree (5) 2. The straw task simulated a technical challenge encountered in clinical practice. 4.5 ± 0.7 4.5 ± 0.6 3. The ball task simulated a technical challenge encountered in clinical practice. 4.4 ± 0.7 4.3 ± 0.5 4. The heel-toe task simulated a technical challenge encountered in clinical practice. 4.6 ± 0.5 4.4 ± 0.7 5. The out-of-plane dowel task simulated a technical challenge encountered in clinical practice. 4.1 ± 0.7 4.9 ± 0.4 6. Although the model does not attempt to simulate true anatomic structures, the haptic feel of the training model approximates that of an actual clinical ultrasound-guided invasive procedure. 4.4 ± 0.6 4.3 ± 0.5 7. Repetitive use of the training model will improve a fellow’s hand-eye coordination with ultrasound needle guidance. 4.8 ± 0.4 4.8 ± 0.4 8. Repetitive use of the training model will improve a fellow’s clinical skill with ultrasound-guided invasive procedures. 4.8 ± 0.4 4.6 ± 0.6 9. Repetitive use of the training model will be useful in fellow training in ultrasound-guided invasive procedures. 4.8 ± 0.4 4.8 ± 0.4 10. If available, I would use the training model in the training of the Maternal-Fetal Medicine fellows I supervise. n/a 4.4 ± 065 11. I recommend that other Maternal-Fetal Medicine fellowship programs use the training model in the training of their fellows. n/a 4.7 ± 0.6 12. Repetitive use of the training model will improve an inexperienced provider’s hand-eye coordination with ultrasound needle guidance. n/a 4.5 ± 0.6 13. Repetitive use of the training model will improve an experienced provider’s clinical skill with ultrasound-guided invasive procedures. n/a 4.5 ± 0.7
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Supplementary Data
Get Radiology Tree app to read full this article<
Video 1
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Video 2
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Video 3
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Video 4
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Video 5
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Leschot N.J., Verjaal M., Treffers P.E.: Risks of midtrimester amniocentesis; assessment in 3000 pregnancies. Br J Obstet Gynaecol 1985; 92: pp. 804-807.
2. Nizard J., Duyme M., Ville Y.: Teaching ultrasound-guided invasive procedures in fetal medicine: learning curves with and without an electronic guidance system. Ultrasound Obstet Gynecol 2002; 19: pp. 274-277.
3. Wijnberger L.D., van der Schouw Y.T., Christiaens G.C.: Learning in medicine: chorionic villus sampling. Prenat Diagn 2000; 20: pp. 241-246.
4. Siragusa D.A., Cardella J.F., Hieb R.A., et. al.: Requirements for training in interventional radiology. J Vasc Interv Radiol 2013; 24: pp. 1609-1612.
5. AIUM : AIUM practice parameter for the performance of selected ultrasound-guided procedures. Available at: http://www.aium.org/resources/guidelines/usGuidedProcedures.pdf Accessed January 25, 2017
6. Cook D.A., Hatala R., Brydges R., et. al.: Technology-enhanced simulation for health professions education a systematic review and meta-analysis. JAMA 2011; 306: pp. 978-988.
7. McGaghie W.C., Issenberg S.B., Cohen E.R., et. al.: Does simulation-based medical education with deliberate practice yield better results than traditional clinical education? A meta-analytic comparative review of the evidence. Acad Med 2011; 86: pp. 706-711.
8. McGaghie W.C., Issenberg S.B., Petrusa E.R., et. al.: Effect of practice on standardised learning outcomes in simulation-based medical education. Med Educ 2006; 40: pp. 792-797.
9. McGaghie W.C., Issenberg S.B., Petrusa E.R., et. al.: A critical review of simulation-based medical education research: 2003–2009. Med Educ 2010; 44: pp. 50-63.
10. American Educational Research Association : Standards for educational and psychological testing.2014.American Educational Research AssociationWashington, DC
11. Zubair I., Marcotte M.P., Weinstein L., et. al.: A novel amniocentesis model for learning stereotactic skills. Am J Obstet Gynecol 2006; 194: pp. 846-848.
12. Wax J.R., Cartin A., Pinette M.G.: The birds and the beans: a low-fidelity simulator for chorionic villus sampling skill acquisition. J Ultrasound Med 2012; 31: pp. 1271-1275.