
Rationale and Objectives
Inguinal lymph nodes can be the first or the only clinical signs of tumor metastases. The aim of the study was to evaluate the role of contrast-enhanced high-resolution magnetic resonance (MR) lymphangiography in diagnosis of inguinal lymph node metastases.
Materials and Methods
The study enrolled 26 patients with inguinal lymph node metastases. Contrast-enhanced lymphangiography was performed using a 3.0T MR unit after intracutaneous injection of gadobenate dimeglumine into the interdigital webs of the dorsal foot. Images of inguinal lymph nodes were acquired before and after contrast injection.
Results
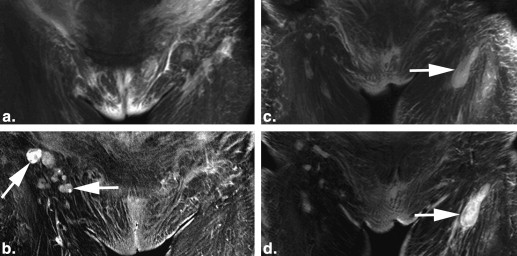
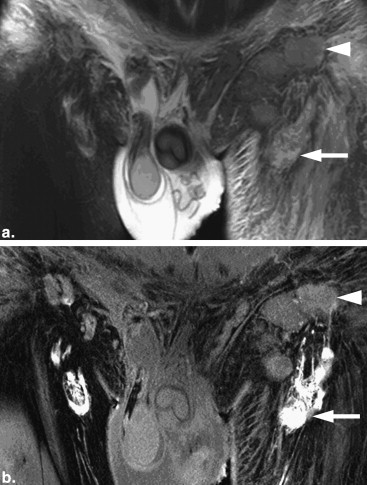
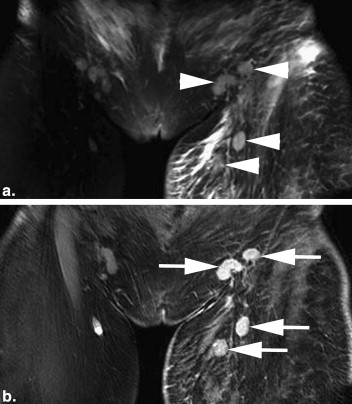
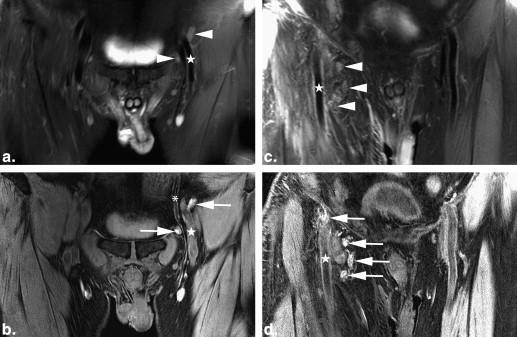
All patients exhibited edema in the subcutaneous layer with significant dilatation of lymphatic collectors in the affected lower limbs on MR images. Before contrast injection, the outline and structure of the affected nodes were unclear on T2 weighted images. Structural changes became evident on postinjection T1-weighted images. Nodal involvement on contrast enhanced MR lymphangiograms was characterized as: 1) heterogeneous structure with partial or marginal enhancement of the node indicating partial occupation by tumor; 2) homogeneous structure of the node without contrast enhancement, indicating total occupation with metastasis, with increase or no change in size; and 3) heterogeneous structure with punctiform nodal enhancement indicating diffuse growth of tumor within the node. Further examinations confirmed the diagnoses of inguinal lymph node metastases of either regional or distal tumors.
Conclusions
Contrast-enhanced high-resolution MR lymphangiography was a sensitive modality in the diagnosis of malignant peripheral lymphedema and the identification of inguinal lymph node metastasis in patients with various tumor origins.
Introduction
The spread of tumors to lymph nodes is an important means of tumor dissemination. Inguinal lymph node metastasis can be a manifestation of different tumor origins. Because of the impairment of lymph backflow within the tumor occupying inguinal metastasis often accompanied by malignant lymphedema of the affected lower limb. Malignant lymphedema could be the first or the only physical sign of tumor metastasis through the lymph nodal pathway and often confused with benign lymphedema, the latter occurs in the extremities because of congenital lymphatic system dysplasia, or acquired lymphatic damage caused by injury, infection, or surgical procedures. Therefore differential diagnosis of benign lymphedema and malignant lymphedema is of primary importance. A sensitive and reliable imaging modality to detect the involved lymph node will be favorable to an earlier diagnosis. Magnetic resonance imaging (MRI) is considered superior to computed tomography (CT) for local staging of carcinoma . Recently, high-resolution MRI with various contrast agents that are injected intravenously has emerged as a new diagnostic method in the clinic. This modality has much higher accuracy rates in detecting nodal metastasis than conventional MRI . High-resolution MR lymphangiography has been proven to be useful in the diagnosis of peripheral lymphatic system disorders in the author’s clinic as well as in other clinics . Based on MR lymphangiography findings in our clinic, 26 patients were diagnosed with inguinal lymph node metastasis and malignant lymphedema of the lower extremities. Further pathological and laboratory tests revealed that tumors that had spread to the inguinal lymph nodes had diverse origins. In all patients, swelling of the lower extremities and external genitalia was the first and/or the only clinical symptom of the disease. All of these patients had been misdiagnosed as benign lymphedema before they came to our clinic. Here, we present the MR lymphangiographic findings and clinical data of these patients.
Materials and methods
Patients
Twenty-six patients with swelling of the lower extremities and external genitalia were included in this study. Among the patients, 8 had bilateral and 18 had unilateral lymphedema. Nine patients also exhibited edema of the external genitalia and/or lower abdominal wall. An inguinal mass (enlarged inguinal lymph nodes) was found in 5 patients. The clinical characteristics of the patients are summarized in Table 1 . Eleven were female and 15 male. The mean age of patients was 55 (range 32–82) years. The mean duration of swelling was 9.75 months (range 1 week–2 years). Eight patients had previously undergone surgical treatment for malignant tumors with various origins.
Table 1
Characteristics of the 26 Patients in the Study
Characteristics Value Age (y) Mean 55 Range 32–82 Duration of disease Mean 9 month Range 1 week to 2 years Inguinal mass 5 Edema in subcutaneous 26 Edema in both subcutaneous and muscle 7 Regional Scrotum Paget’s disease 2 Bladder cancer 1 Prostate cancer 2 Cervical cancer 4 Ovarian cancer 2 Nonregional Liver cancer 1 Non-Hodgkin lymphoma 2 Colon cancer 3 Nasopharynx cancer 1 Gastric cancer 1 Atypical fibrohistiocytoma 1 Gastrointestinal adenocarcinoma of unknown origin 2 Retroperitoneal fibrosis 1 Malignant metastasis of unknown origin 2
Get Radiology Tree app to read full this article<
MR Lymphangiography Test
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Magnetic Resonance Lymphangiographic Findings of Nodal Metastasis in 26 Patients
Inguinal Node Involvement Iliac Node Involvement Superior Group Median (Deep) Group Inferior Group Type of nodal changes Irregular in shape 6 (case) 6 6 No enhancement 16 15 7 1 Partial enhancement 6 7 11 Marginal enhancement 2 Punctiform enhancement 2 2 3 4 Full enhancement 2 2 3 1 Enlargement of affected node 18 18 18 No change in size of affected node 8 8 8
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Ali M., Vinay K.M., Mujtaba H.: Metastatic inguinal lymphadenopathy, presenting as the only physical evidence of recurrent ovarian carcinoma. J Gynecol Surg 2003; 19: pp. 81-83.
2. Zhang Q., Yu J.W., Yang W.L., et. al.: Gastrointestinal stromal tumor of stomach with inguinal lymph nodes metastasis: a case report. World J Gastroenterol 2010; 16: pp. 1808-1810.
3. Hricak H., Dooms G.C., Jeffrey R.B., et. al.: Prostatic carcinoma: staging by clinical assessment, CT and MR imaging. Radiology 1987; 162: pp. 331-336.
4. Harisinghani M.G., Barentsz J., Hahn P.F., et. al.: Noninvasive detection of clinically occult lymph-node metastases in prostate cancer. New Engl J Med 2003; 348: pp. 2491-2499.
5. Jager G.J., Barentsz J.O., Oosterhot G.O., et. al.: Pelvic adenopathy in prostatic and urinary bladder carcinoma: MR imaging with a three-dimensional T1-weighted magnetization-prepared-rapid gradient-echo sequence. AJR Am J Roentgenol 1996; 167: pp. 1503-1507.
6. Weissleder R., Elizondo G., Josephson L., et. al.: Experimental lymph node metastases: enhanced detection with MR lymphography. Radiology 1989; 171: pp. 835-839.
7. Pan D., Suzuki Y., Yang P.C., et. al.: Indirect magnetic resonance lymphangiography to assess lymphatic function in experimental murine lymphedema. Lymph Res Biol 2006; 4: pp. 211-216.
8. Liu N.F., Lu Q., Jiang Z.H., et. al.: Anatomic and functional evaluation of the lymphatics and lymph nodes in diagnosis of lymphatic circulation disorders with contrast magnetic resonance lymphangiography. J Vasc Surg 2009; 49: pp. 980-987.
9. Lu Q., Xu J., Liu N.: Chronic lower extremity lymphedema: a comparative study of high-resolution interstitial MR lymphangiography and heavily T2-weighted MRI. Eur J Radiol 2010; 73: pp. 365-373.
10. McMahon C.J., Rofsky N.M., Pedrosa I.: Lymphatic metastases from pelvic tumor: anatomic classification, characterization, and staging. Radiology 2010; 254: pp. 31-46.
11. Koh D.M., Hughes M., Husband J.E.: Cross-sectional imaging of nodal metastases in the abdomen and pelvis. Abdom Imaging 2006; 31: pp. 632-643.
12. Tobler N.E., Detmar M.: Tumor and lymph node lymphangiogenesis—impact on cancer metastasis. J Leukocyte Biol 2006; 80: pp. 691-696.
13. Tempany C.M., Mcneil B.J.: Advances in biomedical imaging. JAMA 2001; 285: pp. 562-567.
14. Gotoda T., Yanagisawa A., Sasako M., et. al.: Incidence of lymph node metastasis from early gastric cancer: estimation with a large number of cases at two large centers. Gastric Cancer 2000; 3: pp. 219-225.
15. Guarischi A., Keane T.J., Elhakim T.: Metastatic inguinal nodes from an unknown primary neoplasm. a review of 56 cases. Cancer 1987; 59: pp. 572-577.