
Rationale and Objectives
The role of digital breast tomosynthesis (DBT) in evaluating palpable abnormalities has not been evaluated and its accuracy compared to 2D mammography is unknown. The purpose of this study was to evaluate combined 2D mammography, DBT, and ultrasound (US) at palpable sites.
Materials and Methods
Two breast imagers reviewed blinded consecutive cases with combined 2D mammograms and DBT examinations performed for palpable complaints. By consensus, 2D and DBT findings were recorded and compared to US. Patient characteristics, demographics, subsequent workup, and outcome were recorded.
Results
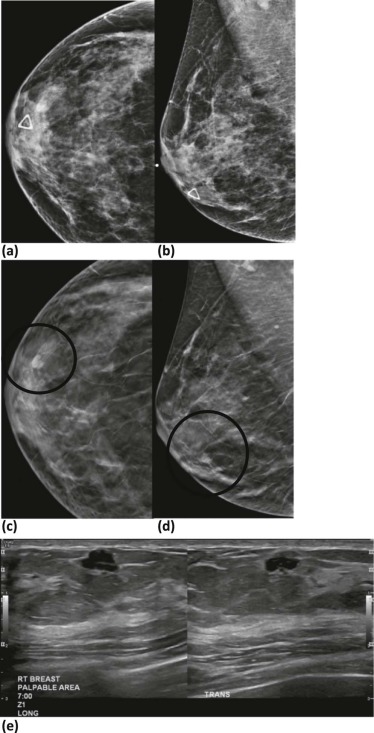
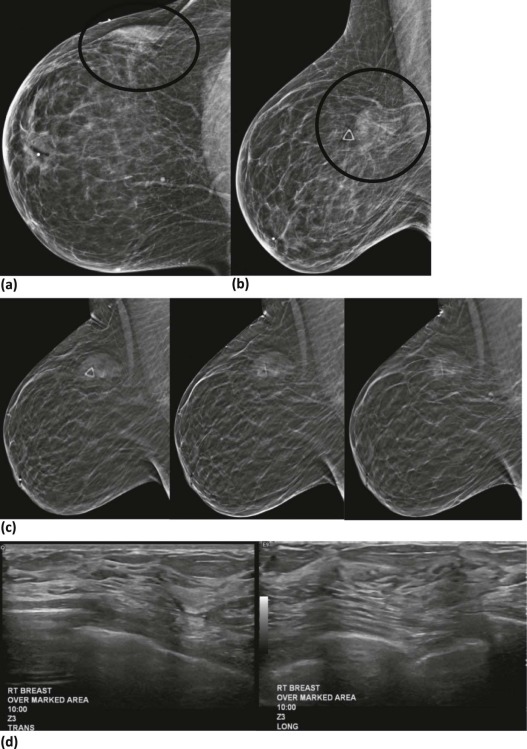
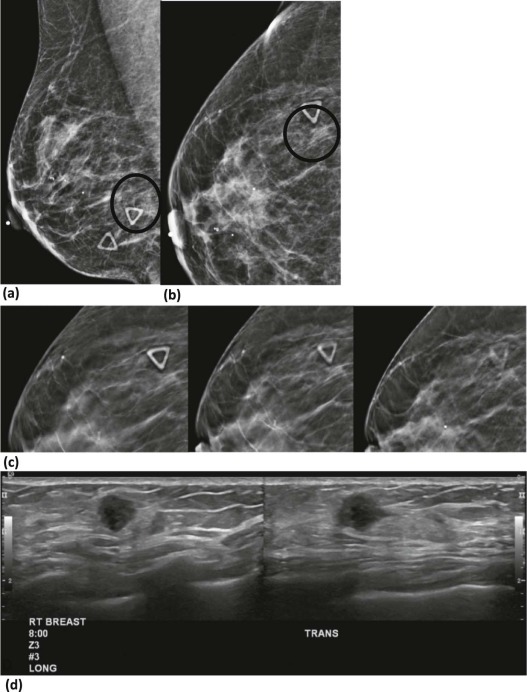
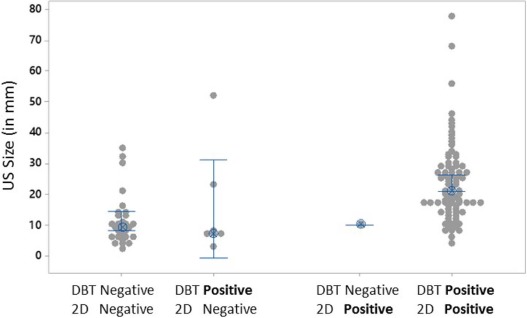
A total of 229 sites in 188 patients were included, with 50 biopsies performed identifying 18 cancers. All 18 cancers were identified on 2D and US, whereas 17 cancers were identified on DBT. Cancer detection sensitivities for 2D, DBT, and US were 100.0%, 94.4%, and 100.0%. The negative predictive value, when combined with US, was 100% for both. The sensitivity and the specificity for both benign and malignant findings with 2D and DBT were 70.5% versus 75.4% ( P = 0.07) and 95.3% versus 99.1% ( P = 0.125). Palpable findings not identified by 2D and DBT were smaller than those identified (11.5 ± 8.3 mm vs 23.9 ± 12.8 mm, P < 0.001). Patients with dense breasts were more likely to have mammographically occult findings than patients with nondense breasts (27.4% vs 8.3%).
Conclusions
DBT did not improve cancer detection over 2D or US. Both mammographic modalities failed to identify sonographically confirmed findings primarily in dense breasts. The diagnostic use of DBT at palpable sites provided limited benefit over combined 2D and US. When utilizing DBT, US should be performed to adequately characterize palpable sites.
Introduction
Palpable abnormalities of the breast are one of the most common indications for which patients present for diagnostic breast imaging. Although most palpable abnormalities are benign, new palpable findings are a common presenting sign of breast cancer . Physical examination of the breast may be difficult as breasts have varying volumes of parenchymal tissues and fat. Previous research has shown that cystic causes of palpable abnormalities cannot be readily distinguished from solid masses by physical examination, and significant disagreement often occurs in the characterization of palpable breast masses even among experienced examiners .
Many breast masses do not exhibit definitive physical findings, and diagnostic breast imaging is often required to differentiate between benign and malignant causes of palpable abnormalities. The American College of Radiology (ACR) publishes appropriateness criteria guiding the recommended imaging examinations performed in the diagnosis of palpable breast masses . Typically, diagnostic imaging evaluations include some combination of mammography and targeted ultrasound (US) depending on patient age. Diagnostic mammography is recommended as the initial imaging step for women aged 40 or greater with palpable breast masses. Women aged 30–39 may either utilize diagnostic mammography or targeted US initially, depending on physician or practice preference. Imaging findings, which are not definitively benign on initial imaging evaluation, typically require additional evaluation with the alternate modality. Women under 30 years of age typically undergo US initially with mammography reserved to clarify indeterminate features or for further evaluation of suspicious findings.
Get Radiology Tree app to read full this article<
Materials and Methods
Study Population
Get Radiology Tree app to read full this article<
Image Interpretation and Acquisition
Get Radiology Tree app to read full this article<
Data Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Clinical Variables
Clinical Variables Patients 188 Palpable events 229 Age (y), mean ± SD 44.7 ± 11.3 Patients with dense breasts \* 124 (66) Patients with nondense breasts \* 64 (34) Palpable events that underwent diagnostic sampling 50 (21.8) Mean follow-up (mo), mean ± SD † 25.7 ± 12.1
SD, standard deviation.
All data except age and mean follow-up reported as the number (%) of patients.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Summary of Results of All Imaging Interpretations
2D Mammography 3D Mammography (DBT) Ultrasound Palpable Cases Cancers − − − 102 (44.5) 0 (0) − −+ 29 (12.7) 0 (0) −+ − 0 (0) 0 (0) −++ 7 (3.1) 0 (0)+ − − 4 (1.7) 0 (0)+ −+ 1 (0.4) 1 (5.6) \* ++ − 1 (0.4) 0 (0)+++ 85 (37.1) 17 (94.4)
DBT, digital breast tomosynthesis.
The + symbol denotes a positive finding was identified and described. The − symbol denotes no finding was identified. All data reported as the number (%) of cases.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Ma I., Dueck A., Gray R., et. al.: Clinical and self breast examination remain important in the era of modern screening. Ann Surg Oncol 2012; 19: pp. 1484-1490.
2. Rosner D., Blaird D.: What ultrasonography can tell in breast masses that mammography and physical examination cannot. J Surg Oncol 1985; 28: pp. 308-313.
3. Boyd N.F., Sutherland H.J., Fish E.B., et. al.: Prospective evaluation of physical examination of the breast. Am J Surg 1981; 142: pp. 331-334.
4. Harvey J.A., Mahoney M.C., Newell M.S., et. al.: ACR appropriateness criteria palpable breast masses. J Am Coll Radiol 2016; 13: pp. e31-e42.
5. Ciatto S., Houssami N.: Breast imaging and needle biopsy in women with clinically evident breast cancer: does combined imaging change overall diagnostic sensitivity?. Breast 2007; 16: pp. 382-386.
6. Murphy I.G., Dillon M.F., Doherty A.O., et. al.: Analysis of patients with false negative mammography and symptomatic breast carcinoma. J Surg Oncol 2007; 96: pp. 457-463.
7. Shetty M.K., Shah Y.P., Sharman R.S.: Prospective evaluation of the value of combined mammographic and sonographic assessment in patients with palpable abnormalities of the breast. J Ultrasound Med 2003; 22: pp. 263-268.
8. Shetty M.K., Shah Y.P.: Prospective evaluation of the value of negative sonographic and mammographic findings in patients with palpable abnormalities of the breast. J Ultrasound Med 2002; 21: pp. 1211-1216.
9. Moy L., Slanetz P.J., Moore R., et. al.: Specificity of mammography and US in the evaluation of a palpable abnormality: retrospective review. Radiology 2002; 225: pp. 176-181.
10. Skaane P., Gullien R., Bjorndal H., et. al.: Digital breast tomosynthesis (DBT): initial experience in a clinical setting. Acta Radiol 2012; 53: pp. 524-529.
11. Bansal G.J., Young P.: Digital breast tomosynthesis within a symptomatic “one-stop breast clinic” for characterization of subtle findings. Br J Radiol 2015; 88: pp. 20140855.
12. Waldherr C., Cerny P., Altermatt H.J., et. al.: Value of one-view breast tomosynthesis versus two-view mammography in diagnostic workup of women with clinical signs and symptoms and in women recalled from screening. AJR Am J Roentgenol 2013; 200: pp. 226-231.
13. Sickles E.A., D’Orsi C.J., Bassett L.W., et. al.: ACR BI-RADS ® mammography..2013.American College of RadiologyReston, VA:
14. Skaane P., Bandos A.I., Gullien R., et. al.: Comparison of digital mammography alone and digital mammography plus tomosynthesis in a population-based screening program. Radiology 2013; 267: pp. 47-56.
15. Friedewald S.M., Rafferty E.A., Rose S.L., et. al.: Breast cancer screening using tomosynthesis in combination with digital mammography. JAMA 2015; 311: pp. 2499-2507.
16. Andersson I., Ikeda D.M., Zackrisson S., et. al.: Breast tomosynthesis and digital mammography: a comparison of breast cancer visibility and BIRADS classification in a population of cancers with subtle mammographic findings. Eur Radiol 2008; 18: pp. 2817-2825.
17. Zuley M.L., Bandos A.I., Ganott M.A., et. al.: Digital breast tomosynthesis versus supplemental diagnostic mammographic views for evaluation of noncalcified breast lesions. Radiology 2013; 266: pp. 89-95.
18. Lei J., Yang P., Zhang L., et. al.: Diagnostic accuracy of digital breast tomosynthesis versus digital mammography for benign and malignant lesions in breasts: a meta-analysis. Eur Radiol 2014; 24: pp. 595-602.
19. Gao Y., Babb J.S., Toth H.K., et. al.: Digital breast tomosynthesis practice patterns following 2011 FDA approval: a survey of breast imaging radiologists. Acad Radiol 2017; 24: pp. 947-953.
20. Tang W., Hu F.X., Zhu H., et. al.: Digital breast tomosynthesis plus mammography, magnetic resonance imaging plus mammography and mammography alone: a comparison of diagnostic performance in symptomatic women. Clin Hemorheol Microcirc 2017; 66: pp. 105-116.
21. Shen Y., Yang Y., Inoue L.Y.T., et. al.: Role of detection method in predicting breast cancer survival: analysis of randomized screening trials. J Natl Cancer Inst 2005; 97: pp. 1195-1203.
22. Mathis K.L., Hoskin T.L., Boughey J.C., et. al.: Palpable presentation of breast cancer persists in the era of screening mammography. J Am Coll Surg 2010; 210: pp. 314-318.
23. Sickles E.A., D’Orsi C.J.: ACR BI-RADS ® follow-up and outcome monitoring..2013.American College of RadiologyReston, VA:
24. Sippo D.A., Kulkarni K., Di Carlo P., et. al.: Metastatic disease to the breast from extramammary malignancies: a multimodality pictorial review. Curr Probl Diagn Radiol 2016; 45: pp. 225-232.
25. Bohman L.G., Bassett L.W., Gold R.H., et. al.: Brest metastases from extramammary malignancies. Radiology 1982; 144: pp. 309-312.
26. Tagliafico A.S., Calabrese M., Mariscotti G., et. al.: Adjunct screening with tomosynthesis or ultrasound in women with mammography-negative dense breasts: interim report of a prospective comparative trial. J Clin Oncol 2016; Epub ahead of print
27. Elmore J.G., Jackson S.L., Abraham L., et. al.: Variability in interpretive performance at screening mammography and radiologists’ characteristics associated with accuracy. Radiology 2009; 253: pp. 641-651.
28. Jackson S.L., Abraham L., Miglioretti D.L., et. al.: Patient and radiologist characteristics associated with accuracy of two types of diagnostic mammograms. AJR Am J Roentgenol 2015; 205: pp. 456-463.