
Rationale and Objectives
Although multiple studies have shown excellent accuracy statistics for noninvasive angiography by coronary computed tomographic angiography (CCTA), most studies comparing nuclear imaging to CCTA were performed on patients already referred for cardiac catheterization, introducing referral and selection bias. This prospective trial evaluated the diagnostic accuracy of 64-row CCTA to detect obstructive coronary stenosis compared to myocardial perfusion imaging (MPI), using quantitative coronary angiography (QCA) as a reference standard.
Materials and Methods
Twelve sites prospectively enrolled 230 patients (49% male, 57.8 years) with chest pain. All patients underwent MPI and CCTA (Lightspeed VCT/Visipaque 320, GE Healthcare, Milwaukee, WI, USA) prior to invasive coronary angiography (ICA). All patients were evaluated, and those found to have either an abnormal MPI or CCTA were clinically referred for ICA. CCTAs were graded on a 15-segment American Heart Association model by three blinded readers for presence of obstructive stenosis (>50% or >70%); MPI was graded by two blinded readers using a 17-segment model for estimation of the % myocardium ischemic or with stress defects. ICAs were independently graded for % stenosis by QCA. The efficacies of MPI and CCTA were assessed including all vessel segments for per-patient and per-vessel analyses.
Results
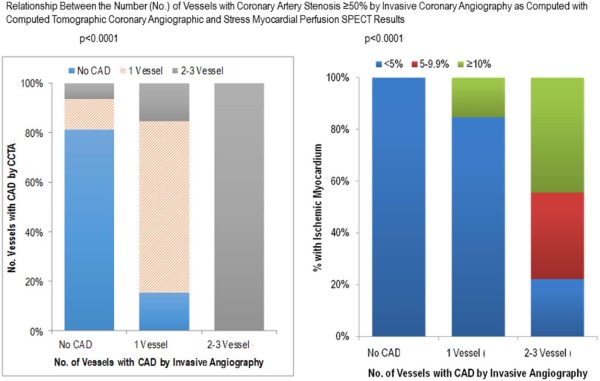
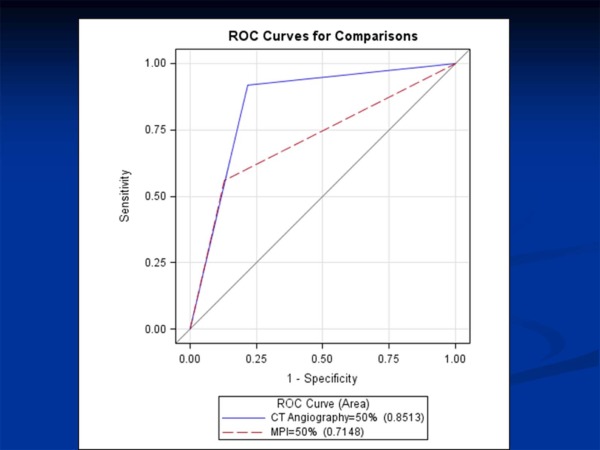
The prevalence of stenosis ≥50% by ICA was 52.1% (25 of 48). The sensitivity of CCTA was significantly higher than nuclear imaging (92.0% vs 54.5%, P < 0.001), with similar specificity (87.0% vs 78.3%) when obstructive disease was defined as ≥50%. CCTA provided superior sensitivity (92.6% vs 59.3%, P < 0.001) and similar specificity (88.9% vs 81.5%) using QCA stenosis ≥70%. For ≥50% stenosis, the computed tomographic angiography odds ratio for ICA disease was 51.75 (95% CI = 8.50–314.94, P < 0.001). For summed stress score ≥5%, the odds ratio for ICA CAD was 12.73 (95% CI = 2.43–66.55, P < 0.001). Using receiver operating characteristic curve analysis, CCTA was better at classifying obstructive coronary artery disease when compared to MPI (area = 0.85 vs 0.71, P < 0.0001).
Conclusions
This study represents one of the first prospective multicenter, controlled clinical trials comparing 64-row CCTA to MPI in the same patients, demonstrating superior diagnostic accuracy of CCTA over myocardial perfusion single photon emission computed tomography (MPS) to reliably detect >50% and >70% stenosis in stable chest pain patients.
Introduction
Although multiple studies have shown excellent accuracy for coronary computed tomographic angiography (CCTA), most studies comparing nuclear imaging with CCTA were performed on patients already referred for cardiac catheterization, introducing selection and referral bias . Stress testing is the most common current noninvasive approach to detecting obstructive coronary artery disease (CAD). Current guidelines recommend functional imaging to risk-stratify and identify patients with higher likelihood of CAD prior to elective coronary angiography. However, a high percentage of patients are found to have nonobstructive CAD . Functional imaging provides physiologic evidence of clinically significant coronary artery stenosis by demonstrating the effects of diminished coronary flow reserve on symptoms leading to myocardial perfusion defects on scintigraphy. Unfortunately, in the United States, a majority of patients who have undergone invasive coronary angiography (ICA) after nuclear testing are found to have nonobstructive or normal coronary arteries, suggesting low diagnostic accuracy of myocardial perfusion imaging (MPI) in current clinical practice . In the National Cath Data Registry (NCDR), stress testing with MPI led to 302,651 patients undergoing ICA, with only 134,670 (44%) demonstrating obstructive disease at ICA. Invasive cardiac catheterization is costly and associated with a small but measurable risk of serious complication due to its invasive nature. In comparison, in the aforementioned NCDR, cardiac computed tomographic angiography (CTA) was performed in 8323 patients and 5791 (70%) were found to have obstructive disease at the time of ICA, representing a 50% improvement in specificity as compared to single photon emission computed tomography (SPECT) MPI. The purpose of this prospective clinical trial is to evaluate the diagnostic accuracy of CCTA to detect obstructive coronary stenosis compared to MPI, using quantitative coronary angiography (QCA) as a reference standard.
Methods
Patient Population
The Perfusion Imaging and CT—Understanding Relative Efficacy (PICTURE) study was a prospective trial with a primary end point to evaluate the diagnostic accuracy of both nuclear imaging and CTA to ICA. Individuals were eligible for participation in the PICTURE trial if they were ≥18 years of age, experienced typical or atypical chest pain, and were being referred for nuclear testing for evaluation of their chest pain. Individuals were excluded from participation in the PICTURE trial for the following reasons: known allergy to iodinated contrast; baseline renal insufficiency (creatinine ≥1.7 mg/dL); irregular cardiac rhythm; resting heart rate >100 beats per minute; resting systolic blood pressure <100 mmHg; contraindication to beta blocker, calcium channel blocker, or nitroglycerin; pregnancy; or known history of CAD (prior myocardial infarction, percutaneous transluminal coronary angioplasty or intracoronary stent, or coronary artery bypass surgery). All patients had to undergo both MPI and CCTA prior to ICA to be enrolled. Importantly, patients were not excluded for elevated coronary artery calcium score or body mass index.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Clinical and Demographic Characteristics of Study Subjects
Total Enrolled ( n = 230) Patients Undergoing QCA Yes ( n = 48) No ( n = 182)P Value Age (years) 57.8 ± 11.4 59.7 ± 12.2 57.2 ± 11.2 0.185 Female, n (%) 113(51.4) 18(37.5) 95(55.2) 0.03 Race/Ethnicity, n (%) 0.305 Caucasian 132(60.0) 34(70.8) 98(57.0) African American 13(5.9) 2(4.2) 11(6.4) Hispanic/Latino 27(12.3) 2(4.2) 25(14.5) Oriental/Asian 34(15.5) 7(14.6) 27(15.7) Others 14(6.4) 3(6.3) 11(6.4) BMI (kg/m 2 ) 30.1 ± 6.9 29.7 ± 6.8 30.2 ± 7.0 0.683 Diabetes, n (%) 38(17.6) 9(18.8) 29(17.3) 0.528 Family history of CAD, n (%) 129(59.7) 31(64.6) 98(58.3) 0.136 Hypertension, n (%) 130(60.2) 27(56.3) 103(61.3) 0.98 Hyperlipidemia, n (%) 126(54.8) 28(58.3) 98(53.8) 0.97 Smoking status, n (%) 0.03 Current smoker 43(19.5) 14(29.2) 29(16.9) Prior smoker 122(55.5) 25(52.1) 97(56.4) Nonsmoker 55(25.0) 9(18.8) 46(26.7)
BMI, body mass index; CAD, coronary artery disease; QCA, quantitative coronary angiography.
Get Radiology Tree app to read full this article<
Rest and Stress MPI Protocol
Get Radiology Tree app to read full this article<
CCTA Image Acquisition
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
CCTA Interpretation
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
ICA Image Acquisition and Interpretation
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Data Analysis
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Clinical Characteristics
Get Radiology Tree app to read full this article<
Prevalence of MPI and CCTA Findings
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Diagnostic Accuracy
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Diagnostic Accuracy Statistics for Coronary Computed Tomographic Angiography and Stress Myocardial Perfusion Imaging (MPI) SPECT in Patients Prospectively Enrolled in the PICTURE Trial Undergoing ICA
% (95% CI) % (95% CI) % (95% CI) % (95% CI) Sensitivity Specificity Positive Predictive Value Negative Predictive Value CT angiography ≥50% 92.0 (74.0, 99.0) 78.3 (56.3, 92.5) 82.1 (63.1, 93.9) 90.0 (68.3, 98.8) ≥70% 92.6 (73.8, 99.0) 88.9 (70.8, 97.7) 84.2 (60.4, 96.6) 82.8 (64.2, 94.2) MPI ≥50% 54.5 (34.9, 75.6) 87.0 (66.4, 97.2) 82.4 (56.6, 96.2) 64.5 (45.4, 80.8) ≥70% 59.3 (34.0, 78.2) 81.5 (61.9, 93.7) 70.6 (44.0, 89.7) 71.0 (52.0, 85.8)
CI, confidence interval; ICA, invasive coronary angiography; PICTURE, Perfusion Imaging and CT–Understanding Relative Efficacy; SPECT, single photon emission computed tomography.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Acknowledgment
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Hamirani Y.S., Isma’eel H., Larijani V., et. al.: The diagnostic accuracy of 64-detector cardiac computed tomography compared with stress nuclear imaging in patients undergoing invasive cardiac catheterization. J Comput Assist Tomogr 2010; 34: pp. 645-651.
2. Budoff M.J., Rasouli M.L., Shavelle D.M., et. al.: Cardiac CT angiography (CTA) and nuclear myocardial perfusion imaging (MPI)-a comparison in detecting significant coronary artery disease. Acad Radiol 2007; 14: pp. 252-257.
3. Budoff M.J., Jacob B., Rasouli M.L., et. al.: Comparison of electron beam computed tomography and technetium stress testing in differentiating cause of dilated versus ischemic cardiomyopathy. J Comput Assist Tomogr 2005; 29: pp. 699-703.
4. Schuijf J.D., Wijns W., Jukema W., et. al.: Relationship between noninvasive coronary angiography with Multislice computed tomography and Myocardial Perfusion Imaging. J Am Coll Cardiol 2006; 48: pp. 2508-2514.
5. Budoff M.J., Achenbach S., Blumenthal R.S., et. al.: Assessment of coronary artery disease by cardiac computed tomography, a scientific statement from the American Heart Association Committee on Cardiovascular Imaging and Intervention, Council on Cardiovascular Radiology and Intervention, and Committee on Cardiac Imaging, Council on Clinical Cardiology. Circulation 2006; 114: pp. 1761-1791.
6. Patel M.R., Dai D., Hernandez A.F., et. al.: Prevalence and predictors of nonobstructive coronary artery disease identified with coronary angiography in contemporary clinical practice. Am Heart J 2014; 167: pp. 846-852.
7. Gerber T.C., Carr J.J., Arai A.E., et. al.: Ionizing radiation in cardiac imaging. a science advisory from the American Heart Association Committee on Cardiac Imaging of the Council on Clinical Cardiology and Committee on Council on Cardiovascular Imaging of the Cardiovascular Radiology and Intervention. Circulation 2009; 119: pp. 1056-1065.
8. Budoff M.J., Dowe D., Jollis J.G., et. al.: Diagnostic performance of 64-multidetector row coronary computed tomographic angiography for evaluation of coronary artery stenosis in individuals without known coronary artery disease: results from the prospective multicenter ACCURACY (Assessment by Coronary Computed Tomographic Angiography of Individuals Undergoing Invasive Coronary Angiography) Trial. J Am Coll Cardiol 2008; 52: pp. 1724-1732.
9. Neglia D., Rovai D., Caselli C., et. al.: Detection of significant coronary artery disease by noninvasive anatomical and functional imaging. Circ Cardiovasc Imaging 2015; 8: pp. e002179.
10. Mark D.B., Berman D.S., Budoff M.J., et. al.: ACCF/ACR/AHA/NASCI/SAIP/SCAI/SCCT 2010 expert consensus document on coronary computed tomographic angiography: a report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents. J Am Coll Cardiol 2010; 55: pp. 2663-2699.
11. Budoff M.J., Liu S., Chow D., et. al.: Coronary CT angiography versus standard of care strategies to evaluate patients with potential coronary artery disease; effect on long term clinical outcomes. Atherosclerosis 2014; 237: pp. 494-498.
12. Nielsen L.H., Ortner N., Nørgaard B.L., et. al.: The diagnostic accuracy and outcomes after coronary computed tomography angiography vs. conventional functional testing in patients with stable angina pectoris: a systematic review and meta-analysis. Eur Heart J Cardiovasc Imaging 2014; 15: pp. 961-971.
13. Budoff M.J., Li D., Coronary C.T.: Angiography again results in better patient outcomes. J Am Coll Cardiol 2014; 64: pp. 741-742.
14. SCOT-HEART Investigators : CT coronary angiography in patients with suspected angina due to coronary heart disease (SCOT-HEART): an open-label, parallel-group, multicentre trial. Lancet 2015; 385: pp. 2383-2391.
15. Douglas P.S., Hoffman U., Patel M.R., et. al.: Outcomes of anatomical versus functional testing for coronary artery disease. N Engl J Med 2015; 372: pp. 1291-1300.
16. Williams M.C., Hunter A., Shah A.S.V., et. al.: Use of coronary computed tomographic angiography to guide management of patients with coronary disease. J Am Coll Cardiol 2016; 67: pp. 1759-1768.
17. Amsterdam E.A., Wenger N.K., Brindis R.G., et. al.: 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2014; 64: pp. e139-e228.