
Rationale and Objectives
To systematically review and meta-analyze published data about the diagnostic accuracy of fluorine-18-fluorodeoxyglucose ( 18 F-FDG) positron emission tomography (PET) and PET/computed tomography (CT) in the differential diagnosis between malignant and benign pleural lesions.
Methods and Materials
A comprehensive literature search of studies published through June 2013 regarding the diagnostic performance of 18 F-FDG-PET and PET/CT in the differential diagnosis of pleural lesions was carried out. All retrieved studies were reviewed and qualitatively analyzed. Pooled sensitivity, specificity, positive and negative likelihood ratio (LR+ and LR−) and diagnostic odds ratio (DOR) of 18 F-FDG-PET or PET/CT in the differential diagnosis of pleural lesions on a per-patient–based analysis were calculated. The area under the summary receiver operating characteristic curve (AUC) was calculated to measure the accuracy of these methods. Subanalyses considering device used (PET or PET/CT) were performed.
Results
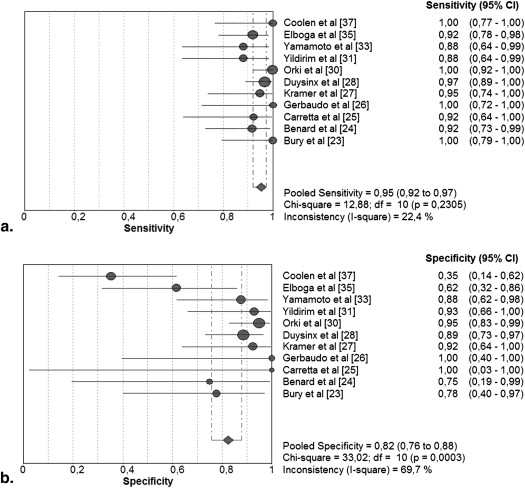
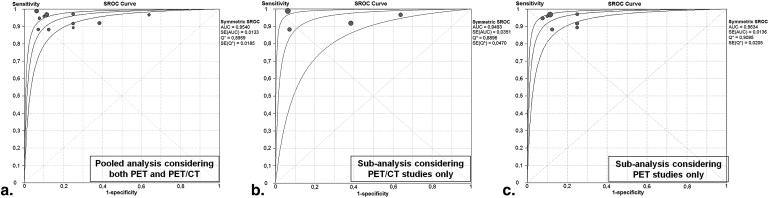
Sixteen studies including 745 patients were included in the systematic review. The meta-analysis of 11 selected studies provided the following results: sensitivity 95% (95% confidence interval [95%CI]: 92–97%), specificity 82% (95%CI: 76–88%), LR+ 5.3 (95%CI: 2.4–11.8), LR− 0.09 (95%CI: 0.05–0.14), DOR 74 (95%CI: 34–161). The AUC was 0.95. No significant improvement of the diagnostic accuracy considering PET/CT studies only was found.
Conclusions
18 F-FDG-PET and PET/CT demonstrated to be accurate diagnostic imaging methods in the differential diagnosis between malignant and benign pleural lesions; nevertheless, possible sources of false-negative and false-positive results should be kept in mind.
Malignant pleural lesions are not uncommon. In 90% of the cases, they are secondary and caused by metastatic disease or lymphoma. In only 10% of the cases, pleural malignancy is primary and caused by malignant pleural mesothelioma or, more rarely, by other primary pleural tumors . The correct differential diagnosis between malignant and benign pleural disease is crucial, because the management and the prognosis of these lesions are different .
Imaging methods may play an important role in the differential diagnosis between malignant and benign pleural lesions . Computed tomography (CT) is the first-line diagnostic method in pleural pathologies . However, this method is not always able to differentiate between malignant and benign pleural lesions because of the significant overlap between the radiological appearances of these conditions .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Methods
Get Radiology Tree app to read full this article<
Search Strategy
Get Radiology Tree app to read full this article<
Study Selection
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Data Extraction
Get Radiology Tree app to read full this article<
Quality Assessment
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Literature Search
Get Radiology Tree app to read full this article<
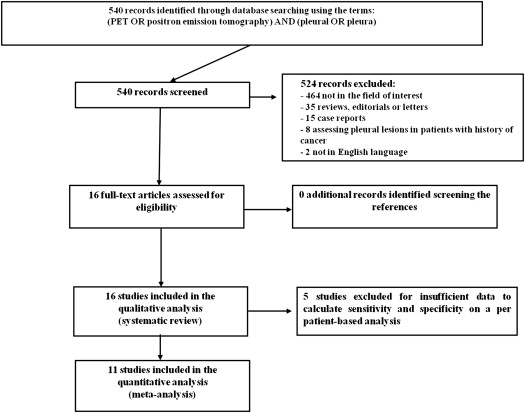
Table 1
Basic Study and Patient Characteristics of the Included Studies
Authors Year Country Study Design Patients Performing 18 F-FDG PET or PET/CT Population Mean Age (y) Gender (%Male) Terada et al 2012 Japan NR 76 Patients with suspicious MPM 67 79 Coolen et al 2012 Belgium Prospective 31 Patients undergoing evaluation for pleural disease 60 77 Abe et al 2012 Japan Retrospective 90 Patients with suspicious MPM NR NR Elboga et al 2012 Turkey Retrospective 50 Patients undergoing evaluation for pleural disease 58 36 Kurata et al 2010 Japan Prospective 17 Patients with suspicious MPM 69 94 Yamamoto et al 2009 Japan Retrospective 33 Patients with suspicious MPM 64 91 Mavi et al 2009 USA NR 55 Patients with suspicious MPM 61 87 Yildirim et al 2009 Turkey NR 31 Patients with suspicious MPM 61 65 Orki et al 2009 Turkey Prospective 83 Patients undergoing evaluation for pleural disease 47 76 Duysinx et al 2006 Belgium Prospective 79 Patients undergoing evaluation for pleural effusions 63 59 Duysinx et al 2004 Belgium Prospective 98 Patients undergoing evaluation for pleural disease 61 68 Kramer et al 2004 Netherlands Prospective 32 Patients undergoing evaluation for pleural disease NR 84 Gerbaudo et al 2002 United States Retrospective 15 Patients with suspicious MPM 60 73 Carretta et al 2000 Italy NR 14 Patients undergoing evaluation for pleural disease 58 79 Bénard et al 1998 United States NR 28 Patients with suspicious MPM NR NR Bury et al 1997 Belgium NR 25 Patients undergoing evaluation for pleural disease 60 NR
CT, computed tomography; 18 F-FDG, fluorine-18-fluorodeoxyglucose; MPM, malignant pleural mesothelioma; NR, not reported; PET, positron emission tomography.
Table 2
Technical Aspects in the Included Studies
Authors Device Mean 18 F-FDG Injected Activity Mean Time between 18 F-FDG Injection and Acquisition (min) Image Analysis Terada et al PET/CT NR 60 Semiquantitative Coolen et al PET/CT 370 MBq 50 Visual Abe et al PET/CT 3.7 MBq/kg 60 and 120 Visual and semiquantitative at early and delayed phase Elboga et al PET/CT 296–555 MBq 60 and 120 Visual and semiquantitative at early and delayed phase Kurata et al PET/CT 5.2 MBq/kg 60 Visual and semiquantitative Yamamoto et al PET 3.5 MBq/kg 60 and 120 Visual and semiquantitative at early and delayed phase Mavi et al PET 5.2 MBq/kg 60 and 90 Semiquantitative at early and delayed phase Yildirim et al PET/CT 350–400 MBq NR Visual and semiquantitative Orki et al PET/CT 370–666 MBq 60–120 Visual and semiquantitative Duysinx et al PET 2.1–3.7 MBq/kg 73 Semiquantitative Duysinx et al PET NR NR Visual Kramer et al PET 400–600 MBq 90 Visual and semiquantitative Gerbaudo et al PET 375 MBq 90 Visual Carretta et al PET 3.7 MBq/kg 60 Visual and semiquantitative Bénard et al PET 4.25 MBq/kg 60–90 Visual and semiquantitative Bury et al PET NR NR Visual
CT, computed tomography; 18 F-FDG, fluorine-18-fluorodeoxyglucose; NR, not reported; PET, positron emission tomography.
Table 3
Diagnostic Accuracy Data of 18 F-FDG PET and PET/CT on a Per-patient–based Analysis Using Visual Analysis at about 1 Hour after 18 F-FDG Injection
Author Number of Cases Final Diagnosis True Positive False Positive True Negative False Negative Sensitivity Specificity Accuracy Positive Predictive Value Negative Predictive Value Malignant Lesions Benign Lesions Terada et al 76 47 29 NR NR NR NR NC NC NC NC NC Coolen et al 31 14 17 14 11 6 0 100% 35% 65% 56% 100% Abe et al 78 31 MPM and 47 non-MPM lesions NR NR NR NR NC NC NC NC NC Elboga et al 50 37 13 34 5 8 3 92% 62% 84% 87% 73% Kurata et al 17 6 11 NR NR NR NR NC NC NC NC NC Yamamoto et al 33 17 16 15 2 14 2 88% 88% 88% 88% 88% Mavi et al 55 44 11 NR NR NR NR NC NC NC NC NC Yildirim et al 31 17 14 15 1 13 2 88% 93% 90% 94% 87% Orki et al 83 44 39 44 2 37 0 100% 95% 98% 96% 100% Duysinx et al 79 51 28 NR NR NR NR NC NC NC NC NC Duysinx et al 98 63 35 61 4 31 2 97% 89% 94% 94% 94% Kramer et al 32 19 13 18 1 12 1 95% 92% 94% 95% 92% Gerbaudo et al , ∗ 15 11 4 11 0 4 0 100% 100% 100% 100% 100% Carretta et al 14 13 1 12 0 1 1 92% 100% 93% 100% 50% Bénard et al 28 24 4 22 1 3 2 92% 75% 89% 96% 60% Bury et al 25 16 9 16 2 7 0 100% 78% 92% 89% 100%
CT, computed tomography; 18 F-FDG, fluorine-18-fluorodeoxyglucose; MPM, malignant pleural mesothelioma; NC, not calculable; NR, not reported; PET, positron emission tomography.
Get Radiology Tree app to read full this article<
Table 4
Quality Assessment of the Included Studies
Author Spectrum of Patients Consecutive or Random Selection of Patients Reference Standard Application of Reference Standard Regardless of Indexed Test Enough Explanation of the Index Test to Ensure Reproducibility Independent Blind Comparison between Index Test and Reference Standard Level of Evidence Abe et al Patients referred because of a clinical diagnosis or suspicion of MPM No Tissue biopsy Yes Yes N/A 3 Bénard et al Patients referred for the evaluation of pleural disease and suspected MPM Yes Tissue biopsy or pleural fluid cytology Clinical follow-up in one. Yes Yes Yes 2 Bury et al Patients undergoing evaluation because of pleural diseases N/A Cytology or tissue biopsy Yes Yes Yes 3 Carretta et al Patients with CT scan evidence of pleural thickening or fluid N/A Tissue biopsy Yes Yes Yes 3 Coolen et al Patients with pleural abnormalities clinically suspicious for malignant pleural diseases Yes Tissue biopsy Yes Yes Yes 2 Duysinx et al Patients presenting exudative pleural effusion and/or pleural thickening Yes Cytologic and histologic methods as well as radiological follow-up Yes Yes Yes 2 Duysinx et al Patients presenting with an exudative pleural effusion after thoracocentesis Yes Pleural biopsy as well as follow-up Yes Yes N/A 3 Elboga et al Patients with pleural pathologies such as pleural mass, pleural thickening, and pleural effusion N/A Surgical biopsy Yes Yes N/A 3 Gerbaudo et al Patients with clinical and radiographic suspicion of malignant mesothelioma Yes Histopathology Yes Yes N/A 3 Kramer et al Patients who had pleural abnormalities and presented at the pulmonary outpatient department (age >18 y) Yes Pleural fluid cytology or pleural biopsies as well as follow-up Yes Yes Yes 2 Kurata et al Patients with asbestos-related pleural disease and suspected MPM Yes Pleural fluid cytology or pleural biopsies as well as follow-up Yes Yes N/A 3 Mavi et al Patients of suspected MPM and recurrence of MPM Yes Histopathology Yes Yes N/A 3 Orki et al Patients with pleural lesions (63 with pleural effusion, 20 with pleural thickening) on CT scan Yes Histopathology Yes Yes N/A 3 Terada et al Patients with confirmed MPM N/A Histopathology or cytology Yes Yes N/A 3 Yamamoto et al Patients who were suspected of having MPM on CT N/A Histopathology or follow-up No (patients with negative PET did not undergo invasive procedures) Yes Yes 4 Yildirim et al Patients with pleural effusions or pleural thickening Yes Histopathology or follow-up Yes Yes No 3
CT, computed tomography; 18 F-FDG, fluorine-18-fluorodeoxyglucose; MPM, malignant pleural mesothelioma; N/A, not available; PET, positron emission tomography.
Get Radiology Tree app to read full this article<
Qualitative Analysis (Systematic Review)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Quantitative Analysis (Meta-analysis)
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
References
1. Feragalli B., Storto M.L., Bonomo L.: Malignant pleural disease. Radiol Med 2003; 105: pp. 266-288.
2. Qureshi N.R., Gleeson F.V.: Imaging of pleural disease. Clin Chest Med 2006; 27: pp. 193-213.
3. Metintas M., Ucgun I., Elbek O., et. al.: Computed tomography features in malignant pleural mesothelioma and other commonly seen pleural diseases. Eur J Radiol 2002; 41: pp. 1-9.
4. Metintas M., Ak G., Parspour S., et. al.: Local recurrence of tumor at sites of intervention in malignant pleural mesothelioma. Lung Cancer 2008; 61: pp. 255-261.
5. Francis R., Segard T., Morandeau L.: Novel molecular imaging in lung and pleural diseases. Respirology 2011; 16: pp. 1173-1188.
6. Treglia G., Cason E., Fagioli G.: Recent applications of nuclear medicine in diagnostics (first part). Ital J Med 2010; 4: pp. 84-91.
7. Duysinx B., Corhay J.L., Larock M.P., et. al.: Contribution of positron emission tomography in pleural disease. Rev Mal Respir 2010; 27: pp. e47-e53.
8. Liberati A., Altman D.G., Tetzlaff J., et. al.: The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol 2009; 62: pp. e1-e34.
9. Oxford Center for Evidence-Based Medicine checklist for diagnostic studies appraisal. Available at: http://www.cebm.net/index.aspx?o_1025 . Accessed June 30, 2013.
10. Egger M., Davey Smith G., Schneider M., et. al.: Bias in meta-analysis detected by a simple, graphical test. BMJ 1997; 315: pp. 629-634.
11. Duval S., Tweedie R.: Trim and fill: a simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000; 56: pp. 455-463.
12. Zamora J., Abraira V., Muriel A., et. al.: Meta-DiSc: a software for meta-analysis of test accuracy data. BMC Med Res Methodol 2006; 6: pp. 31.
13. Erasmus J.J., McAdams H.P., Rossi S.E., et. al.: FDG PET of pleural effusions in patients with non-small cell lung cancer. AJR Am J Roentgenol 2000; 175: pp. 245-249.
14. Gupta N.C., Rogers J.S., Graeber G.M., et. al.: Clinical role of F-18 fluorodeoxyglucose positron emission tomography imaging in patients with lung cancer and suspected malignant pleural effusion. Chest 2002; 122: pp. 1918-1924.
15. Schaffler G.J., Wolf G., Schoellnast H., et. al.: Non-small cell lung cancer: evaluation of pleural abnormalities on CT scans with 18F FDG PET. Radiology 2004; 231: pp. 858-865.
16. Toaff J.S., Metser U., Gottfried M., et. al.: Differentiation between malignant and benign pleural effusion in patients with extra-pleural primary malignancies: assessment with positron emission tomography-computed tomography. Invest Radiol 2005; 40: pp. 204-209.
17. Kim B.S., Kim I.J., Kim S.J., et. al.: Predictive value of F-18 FDG PET/CT for malignant pleural effusion in non-small cell lung cancer patients. Onkologie 2011; 34: pp. 298-303.
18. Alkhawaldeh K., Biersack H.J., Henke A., et. al.: Impact of dual-time-point F-18 FDG PET/CT in the assessment of pleural effusion in patients with non-small-cell lung cancer. Clin Nucl Med 2011; 36: pp. 423-428.
19. Letovanec I., Allenbach G., Mihaescu A., et. al.: 18 F-fluorodeoxyglucose PET/CT findings in pleural effusions of patients with known cancer. A cytopathological correlation. Nuklearmedizin 2012; 51: pp. 186-193.
20. Liao R., Yang X., Wang S., et. al.: Clinical role of F-18 FDG PET/CT in differentiating malignant and benign pleural effusion in patients with lung cancer. Zhongguo Fei Ai Za Zhi 2012; 15: pp. 652-655.
21. Balogova S., Grahek D., Kerrou K., et. al.: [18F]-FDG imaging in apparently isolated pleural lesions. Rev Pneumol Clin 2003; 59: pp. 275-288.
22. Buchmann I., Guhlmann C.A., Elsner K., et. al.: F-18-FDG PET for primary diagnosis differential diagnosis of pleural processes. Nuklearmedizin 1999; 38: pp. 319-322.
23. Bury T., Paulus P., Dowlati A., et. al.: Evaluation of pleural diseases with FDG-PET imaging: preliminary report. Thorax 1997; 52: pp. 187-189.
24. Bénard F., Sterman D., Smith R.J., et. al.: Metabolic imaging of malignant pleural mesothelioma with fluorodeoxyglucose positron emission tomography. Chest 1998; 114: pp. 713-722.
25. Carretta A., Landoni C., Melloni G., et. al.: 18-FDG positron emission tomography in the evaluation of malignant pleural diseases - a pilot study. Eur J Cardiothorac Surg 2000; 17: pp. 377-383.
26. Gerbaudo V.H., Sugarbaker D.J., Britz-Cunningham S., et. al.: Assessment of malignant pleural mesothelioma with (18)F-FDG dual-head gamma-camera coincidence imaging: comparison with histopathology. J Nucl Med 2002; 43: pp. 1144-1149.
27. Kramer H., Pieterman R.M., Slebos D.J., et. al.: PET for the evaluation of pleural thickening observed on CT. J Nucl Med 2004; 45: pp. 995-998.
28. Duysinx B., Nguyen D., Louis R., et. al.: Evaluation of pleural disease with 18-fluorodeoxyglucose positron emission tomography imaging. Chest 2004; 125: pp. 489-493.
29. Duysinx B.C., Larock M.P., Nguyen D., et. al.: 18F-FDG PET imaging in assessing exudative pleural effusions. Nucl Med Commun 2006; 27: pp. 971-976.
30. Orki A., Akin O., Tasci A.E., et. al.: The role of positron emission tomography/computed tomography in the diagnosis of pleural diseases. Thorac Cardiovasc Surg 2009; 57: pp. 217-221.
31. Yildirim H., Metintas M., Entok E., et. al.: Clinical value of fluorodeoxyglucose-positron emission tomography/computed tomography in differentiation of malignant mesothelioma from asbestos-related benign pleural disease: an observational pilot study. J Thorac Oncol 2009; 4: pp. 1480-1484.
32. Mavi A., Basu S., Cermik T.F., et. al.: Potential of dual time point FDG-PET imaging in differentiating malignant from benign pleural disease. Mol Imaging Biol 2009; 11: pp. 369-378.
33. Yamamoto Y., Kameyama R., Togami T., et. al.: Dual time point FDG PET for evaluation of malignant pleural mesothelioma. Nucl Med Commun 2009; 30: pp. 25-29.
34. Kurata S., Ishibashi M., Azuma K., et. al.: Preliminary study of positron emission tomography/computed tomography and plasma osteopontin levels in patients with asbestos-related pleural disease. Jpn J Radiol 2010; 28: pp. 446-452.
35. Elboga U., Yılmaz M., Uyar M., et. al.: The role of FDG PET-CT in differential diagnosis of pleural pathologies. Rev Esp Med Nucl Imagen Mol 2012; 31: pp. 187-191.
36. Abe Y., Tamura K., Sakata I., et. al.: Clinical implications of 18F-fluorodeoxyglucose positron emission tomography/computed tomography at delayed phase for diagnosis and prognosis of malignant pleural mesothelioma. Oncol Rep 2012; 27: pp. 333-338.
37. Coolen J., De Keyzer F., Nafteux P., et. al.: Malignant pleural disease: diagnosis by using diffusion-weighted and dynamic contrast-enhanced MR imaging–initial experience. Radiology 2012; 263: pp. 884-892.
38. Terada T., Tabata C., Tabata R., et. al.: Clinical utility of 18-fluorodeoxyglucose positron emission tomography/computed tomography in malignant pleural mesothelioma. Exp Ther Med 2012; 4: pp. 197-200.
39. Treglia G., Sadeghi R.: Meta-analyses and systematic reviews on PET and PET/CT in oncology: the state of the art. Clin Transl Imaging 2013; 1: pp. 73-75.
40. Spitilli M.G., Treglia G., Calcagni M.L., et. al.: Malignant pleural mesothelioma: utility of 18 F-FDG PET. Ann Ital Chir 2007; 78: pp. 393-396.