
Rationale and Objectives
Given the significance of coronary artery disease as the most important socioeconomic health care problem in the Western World, the application of computer-aided simple triage (CAST) systems to this disease would be desirable.
Materials and Methods
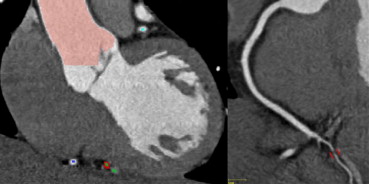
In total, 93 patients with acute chest pain and an intermediate risk score for acute coronary syndrome underwent coronary computed tomography angiography (cCTA). Among those, 74 were of adequate image quality for automated analysis by a commercially available CAST system (COR Analyzer, RCADIA, Haifa, Israel). CAST findings were compared to human expert interpretation for the detection of significant stenosis (≥50%) in the left main, left anterior descending, circumflex, right coronary artery, or arterial branches. Further, one inexperienced observer evaluated all studies for significant stenoses alone and after 1 month guided by a CAST system as an initial read.
Results
Human expert interpretation identified 37/74 patients with stenosis ≥50%, whereas the CAST detected 45 patients. The CAST system demonstrated a sensitivity of 100%/79% and a specificity of 78%/89% on a per-patient/per-vessel level, respectively. With CAST, the inexperienced readers’ per-vessel sensitivity and positive predictive values significantly improved ( P = .011, P = .009) from 69% and 41% to 91% and 74%, respectively.
Conclusions
The investigated CAST system for automatic stenosis detection can accurately identify patients with coronary artery stenosis ≥50% and may be of use as initial interpretation and triage of cCTA studies as well as a second reader for inexperienced readers, in absence of expert readers.
Proper assessment of patients who present with undefined chest pain represents a major challenge for emergency department (ED) physicians. For patients with acute chest pain and a low- to intermediate-risk profile for acute coronary syndrome (ACS), the current guidelines recommend noninvasive diagnostic testing . Several studies have evaluated coronary computed tomography angiography (cCTA) for the detection of significant coronary artery stenosis in comparison with coronary catheterization and consistently report high accuracy . Most important for clinical practice is the high negative predictive value (NPV) of this test, indicating that cCTA can reliably exclude significant coronary artery stenosis . However, a major limitation of cCTA for evaluation of chest pain patients in the ED is the lack of available experienced readers, especially during nighttime and weekend hours. Therefore, a computer-aided detection (CAD) system with consistent performance for coronary artery stenosis detection appears desirable. Although there exist a great variety of automated software tools to assist physicians in manual interpretation of cCTA studies , none of them is able to perform a fully automatic evaluation of a study without human reader interaction. Recently a computer-aided simple triage (CAST) system, which is a subclass of CAD, was introduced . Because of a higher diagnostic accuracy, CAST is aimed to provide a fully automatic initial interpretation of a study: a “wet read.” Unlike conventional CAD systems, primarily used as “second readers,” CAST is able to perform initial study triage automatically. Reliable automatic study triage provided by CAST, followed by human verification performed by a trained physician, could safely exclude ACS and, thus, markedly expand the impact of cCTA on management of acute chest pain.
The aim of this study was to evaluate the diagnostic accuracy of commercially available CAST system for stenosis detection in cCTA and the effect of such a system on the performance of readers with different experience levels in a consecutive cohort of ED patients with an intermediate risk for ACS.
Materials and methods
Study Population
Get Radiology Tree app to read full this article<
Table 1
Baseline Characteristics of Study Population ( n = 93)
Mean Age 59 (27–95) Male 48 (52%) Female 45 (48%) Diabetes mellitus 21 (23%) Hypertension 56 (60%) Hyperlipidemia 27 (29%) BMI 31 (33%) Current smoker 52 (56%) Family history of early CAD 22 (24%) Obesity 46 (50%) Prior CAD 8 (9%) Prior MI within 6 month 3 (3%) Prior PCI within 6 month 2 (21%) Prior Stroke within 6 month 3 (3%) Chest pain “de novo” 43 (46%)
BMI, body mass index; CAD, coronary artery disease; MI, myocardial infarction; PCI, percutaneous coronary intervention.
Numbers in parentheses represent value range.
Get Radiology Tree app to read full this article<
cCTA Image Acquisition
Get Radiology Tree app to read full this article<
cCTA Analysis
Get Radiology Tree app to read full this article<
CAST Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Per-Vessel Analysis
Get Radiology Tree app to read full this article<
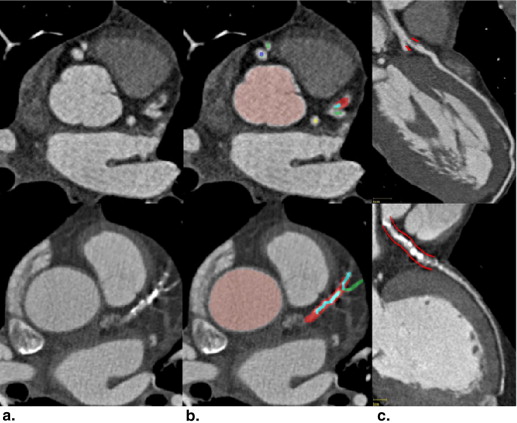
Table 2
Performance Characteristics of the Automated COR Analyzer Algorithm for Detecting Significant Stenosis Compared with cCTA on a Per-vessel and Per-patient Basis
Sensitivity Specificity PPV NPV Per vessel LM 33% (2–88%) 92% (83–97%) 17% (9–64%) 97% (88–100%) LAD 92% (72–99%) 90% (77–96%) 82% (63–93%) 96% (84–99%) LCx 54% (26–80%) 92% (81–97%) 58% (29–84%) 90% (79–96%) RCA 73% (39–92%) 84% (72–92%) 44% (22–69%) 95% (84–99%) Branch vessels 71% (30–95%) 98% (94–99%) 56% (23–85%) 99% (96–100%) Per-patient 100% (88–100%) 78% (61–90%) 82% (67–92%) 100% (85–100%)
AUC, area under the curve; cCTA, coronary computed tomography angiography; LAD, left anterior descending artery; LCx, left circumflex artery; LM, left main artery; NPV, negative predictive value; PPV, positive predictive value; RCA, right coronary artery.
Numbers in parentheses represent 95% confidence interval values.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Performance Characteristics of the Automated COR Analyzer Algorithm for Detecting Significant Stenosis Compared with cCTA on a Per-vessel and Per-patient Bias for an Inexperienced Reader without and with COR Analyzer Algorithm
Sensitivity Specificity PPV NPV Inexperienced Reader without COR Analyzer Algorithm Per vessel LM 67% (13–98%) 89% (79–95%) 20% (4–56%) 98% (91–100%) LAD 83% (62–95%) 76% (62–87%) 63% (44–78%) 91% (77–97%) LCx 54% (26–80%) 82% (70–90%) 39% (18–64%) 89% (77–96%) RCA 64% (32–88 %) 78% (65–87%) 33% (16–57%) 93% (81–98%) Branch vessels 57% (20–88%) 93% (89–96%) 24% (8–50%) 98% (95–100%) Per-patient 94% (81–99%) 70% (53–84%) 76% (61–73%) 93% (75–99%) Inexperienced reader with COR Analyzer algorithm Per vessel LM 100% (31–100%) 92% (82–97%) – – LAD 96% (78–100%) 96% (85–99%) 92% (73–99%) 98% (88–100%) LCx 85% (54–97%) 93% (83–98%) 73% (45–91%) 97% (87–99%) RCA 91% (57–100%) 92% (82–97%) 67% (39–87%) 98% (90–100%) Branch vessels 86% (42–99%) 99% (96–100%) 75% (36–96%) 99% (97–100%) Per-patient 100% (88–100%) 81% (64–91%) 84% (69–93%) 100% (85–100%)
AUC, area under the curve; cCTA, coronary computed tomography angiography; LAD, left anterior descending artery; LCx, left circumflex artery; LM, left main artery; NPV, negative predictive value; PPV, positive predictive value; RCA, right coronary artery.
Numbers in parentheses represent 95% confidence interval values.
Get Radiology Tree app to read full this article<
Per-Patient Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
False-Positives Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Hendel R.C., Patel M.R., Kramer C.M., et. al.: ACCF/ACR/SCCT/SCMR/ASNC/NASCI/SCAI/SIR 2006 appropriateness criteria for cardiac computed tomography and cardiac magnetic resonance imaging: a report of the American College of Cardiology Foundation Quality Strategic Directions Committee Appropriateness Criteria Working Group, American College of Radiology, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, American Society of Nuclear Cardiology, North American Society for Cardiac Imaging, Society for Cardiovascular Angiography and Interventions, and Society of Interventional Radiology. J Am Coll Cardiol 2006; 48: pp. 1475-1997.
2. Anderson J.L., Adams C.D., Antman E.M., et. al.: ACC/AHA 2007 guidelines for the management of patients with unstable angina/non-ST-Elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non-ST-Elevation Myocardial Infarction) developed in collaboration with the American College of Emergency Physicians, the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation and the Society for Academic Emergency Medicine. J Am Coll Cardiol 2007; 50: pp. e1-e157.
3. Schoepf U.J., Zwerner P.L., Savino G., et. al.: Coronary CT angiography. Radiology 2007; 244: pp. 48-63.
4. Vanhoenacker P.K., Heijenbrok-Kal M.H., Van Heste R., et. al.: Diagnostic performance of multidetector CT angiography for assessment of coronary artery disease: meta-analysis. Radiology 2007; 244: pp. 419-428.
5. Raff G.L., Gallagher M.J., O’Neill W.W., et. al.: Diagnostic accuracy of noninvasive coronary angiography using 64-slice spiral computed tomography. J Am Coll Cardiol 2005; 46: pp. 552-557.
6. Isgum I., Rutten A., Prokop M., et. al.: Detection of coronary calcifications from computed tomography scans for automated risk assessment of coronary artery disease. Med Phys 2007; 34: pp. 1450-1461.
7. Reimann A.J., Tsiflikas I., Brodoefel H., et. al.: Efficacy of computer aided analysis in detection of significant coronary artery stenosis in cardiac using dual source computed tomography. Int J Cardiovasc Imaging 2009; 25: pp. 195-203.
8. Sugahara T., Yamagihara Y., Sugimoto N., et. al.: Computer-aided interpretation of coronary cineangiograms. Accuracy of automatic detection of stenotic lesions. Acta Radiol 1992; 33: pp. 6-9.
9. Goldenberg R., Peled N.: Computer-aided simple triage. Int J Comput Assist Radiol Surg 2011; 6: pp. 705-711.
10. Antman E.M., Cohen M., Bernink P.J., et. al.: The TIMI risk score for unstable angina/non-ST elevation MI: A method for prognostication and therapeutic decision making. JAMA 2000; 284: pp. 835-842.
11. Budoff M.J., Achenbach S., Berman D.S., et. al.: Task force 13: training in advanced cardiovascular imaging (computed tomography) endorsed by the American Society of Nuclear Cardiology, Society of Atherosclerosis Imaging and Prevention, Society for Cardiovascular Angiography and Interventions, and Society of Cardiovascular Computed Tomography. J Am Coll Cardiol 2008; 51: pp. 409-414.
12. Austen W.G., Edwards J.E., Frye R.L., et. al.: A reporting system on patients evaluated for coronary artery disease. Report of the Ad Hoc Committee for Grading of Coronary Artery Disease, Council on Cardiovascular Surgery, American Heart Association. Circulation 1975; 51: pp. 5-40.
13. Hawass N.E.: Comparing the sensitivities and specificities of two diagnostic procedures performed on the same group of patients. Br J Radiol 1997; 70: pp. 360-366.
14. Kelm B.M., Mittal S., Zheng Y., et. al.: Detection, grading and classification of coronary stenoses in computed tomography angiography. Med Image Comput Comput Assist Interv 2011; 14: pp. 25-32.
15. Halpern E.J., Halpern D.J.: Diagnosis of coronary stenosis with CT angiography comparison of automated computer diagnosis with expert readings. Acad Radiol 2011; 18: pp. 324-333.
16. Hamon M., Morello R., Riddell J.W.: Coronary arteries: diagnostic performance of 16- versus 64-section spiral CT compared with invasive coronary angiography–meta-analysis. Radiology 2007; 245: pp. 720-731.
17. Arnoldi EM, Schoepf UJ, Rosenblum MA, et al. Computer-aided detection of coronary artery stenosis at computed tomography angiography: effect on performance of readers with different experience levels. Book Computer-aided Detection of Coronary Artery Stenosis at Computed Tomography Angiography: Effect on Performance of Readers with Different Experience Levels. City2010 Abstract. http://ipp.myesr.org/esr/ecr2011/index.php?v=sessiond&seid=215&ippwwwsid=q12crha4f6ckuvv6gsfk3hhid1#pap2561
18. Renker M., Nance J.W., Schoepf U.J., et. al.: Evaluation of heavily calcified vessels with coronary CT angiography: comparison of iterative and filtered back projection image reconstruction. Radiology 2011; 260: pp. 390-399.
19. Hoffmann U., Bamberg F., Chae C.U., et. al.: Coronary computed tomography angiography for early triage of patients with acute chest pain: the ROMICAT (Rule Out Myocardial Infarction using Computer Assisted Tomography) trial. J Am Coll Cardiol 2009; 53: pp. 1642-1650.
20. Hoffmann U., Nagurney J.T., Moselewski F., et. al.: Coronary multidetector computed tomography in the assessment of patients with acute chest pain. Circulation 2006; 114: pp. 2251-2260.
21. Sato Y., Matsumoto N., Ichikawa M., et. al.: Efficacy of multislice computed tomography for the detection of acute coronary syndrome in the emergency department. Circ J 2005; 69: pp. 1047-1051.