
Rationale and Objectives
This study aimed to compare the diagnostic value of automated breast volume scanning (ABVS) to that of handheld ultrasonography (HHUS) using breast magnetic resonance imaging (MRI) as the gold standard.
Materials and Methods
Twenty-eight patients with 39 examined breasts with at least one lesion visible in breast MRI underwent HHUS and ABVS. Detection rate, localization, maximum diameter, and Breast Imaging Reporting and Data System classification were compared. Sensitivity, specificity, diagnostic accuracy, positive predictive value, and negative predictive value were calculated for HHUS and ABVS. Lesion localization and maximum diameters based on HHUS and ABVS were compared to size measurement in MRI. Breast Imaging Reporting and Data System categories based on each method were compared to the MRI diagnosis (malignant or benign) or, if available (21 cases), with the histologic diagnosis.
Results
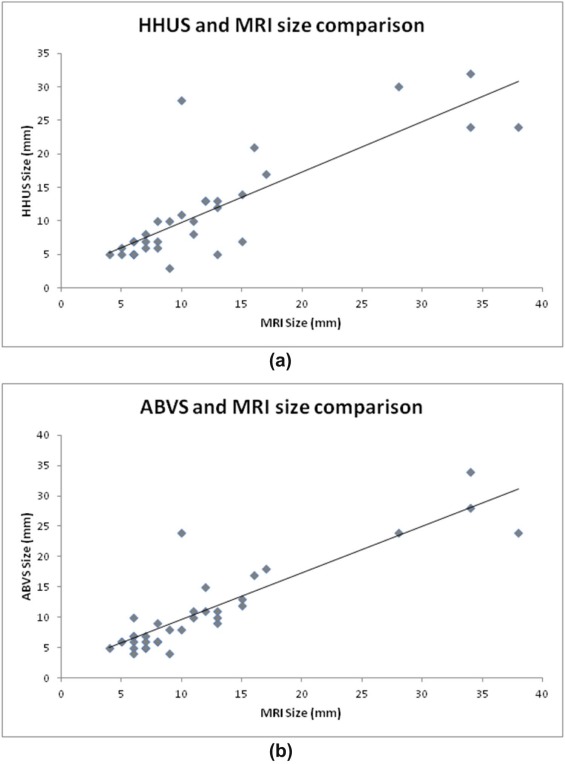
MRI detected 72 lesions, ABVS 59 lesions, and HHUS 54 lesions. Malignancy was proven histopathologically in 15 cases. There was no significant difference between ABVS and HHUS in terms of sensitivity (93.3% vs. 100%), specificity (83.3% vs. 83.3%), diagnostic accuracy (87.2% vs. 89.7%), positive predictive value (77.8% vs. 78.9%), and negative predictive value (95.2% vs. 100%). Agreement regarding lesion localization (same quadrant) was 94.3% for ABVS and MRI and 91.2% for HHUS and MRI. Lesion size compared to MRI lesion size was assessed correctly (+/− 3 mm) in 79.4% (HHUS) and 80% (ABVS). The correlation of size measurement was slightly higher for ABVS-MRI (r = 0.89) than for HHUS-MRI (r = 0.82) with P < .001.
Conclusions
ABVS can be used as an alternative to HHUS. ABVS has the advantage of operator independence and better reproducibility although it is limited in evaluating axillary lymph nodes and lacks Doppler or elastrography capabilities, which sometimes provide important supplementary information in HHUS.
Introduction
Magnetic resonance imaging of the breast (breast MRI) is typically performed in women at higher risk for breast cancer (eg BRCA-1 or BRCA-2 mutation). In Germany, most of these women are enrolled in special breast cancer screening programs, which include a breast MRI examination once a year . Other indications for breast MRI are inconclusive findings of mammography and handheld ultrasonography (HHUS) or the need to evaluate preoperative tumor extent, for example, in case of multifocality. Although breast MRI is highly sensitive, it has variable specificity and a high false-positive rate . Therefore, two-dimensional HHUS is also used as a second-look imaging test to reduce the false-positive rate, by easily identifying lymph nodes or fibroadenomas, classified as nonspecific enhancing lesions by MRI . The other advantage of second-look ultrasound is that it can help in deciding about the biopsy guidance method (ultrasound or MRI). Ultrasound-guided biopsy is preferred to MRI-guided biopsy and can be performed whenever the suspicious breast lesion is detectable by ultrasound . However, because HHUS is very operator-dependent, nonreproducible, and inefficient in the diagnosis of some breast malignancies (especially ductal carcinoma in situ [DCIS]) , the present study was conducted to investigate whether an automated breast volume scanner (ABVS) could overcome these limitations of HHUS.
The ABVS acquires a whole series of consecutive B-mode images by scanning the whole breast in a straight line in anterior-posterior, lateral, and medial directions (and if necessary, eg in women with large breasts, additionally in superior and inferior directions). The acquired images are sent to a separate workstation and are then used to reconstruct three-dimensional (3D) datasets of the entire breast volume including coronal, axial, and sagittal views. The resulting datasets can then be analyzed by a radiologist. Thus, ABVS provides consistent, reproducible, and operator-independent ultrasound imaging of the entire breast . The examination takes 10 minutes and can be performed by a technologist. Interpretation by a radiologist at the workstation takes another 5 minutes .
Materials and Methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
![Figure 1, Invasive ductal carcinoma in a 49-year-old woman. (a) Automated breast volume scanning (ABVS) in the transverse plane ( upper ), sagittal plane ( lower right ), and coronal reconstruction ( lower left ); (b) handheld ultrasonography (HHUS); (c) magnetic resonance imaging (MRI) (axial dynamic three-dimensional gradient-recalled echo [3D GRE] after intravenous administration of gadolinium-based contrast medium).](https://storage.googleapis.com/dl.dentistrykey.com/clinical/DiagnosticPerformanceofAutomatedBreastVolumeScanningABVSComparedtoHandheldUltrasonographyWithBreastMRIastheGoldStandard/0_1s20S1076633217300752.jpg)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Histologic Diagnosis of 21 Lesions
Histologic Diagnosis Number Ductal carcinoma in situ 1 Invasive ductal carcinoma 10 Invasive lobular carcinoma 2 Invasive medullary carcinoma 1 Invasive carcinoma of no special type 1 Fibrocystic mastopathia 4 Microglandular adenosis 2
Table 2
Basic Lesion Features
No. in MRI Average Size in Millimeter Enhancement in MRI Enhancement Initial Phase Delayed Phase ABVS HHUS MRI Fast Medium Slow Washout Plateau Persistent Histologic diagnosis Ductal carcinoma in situ 1 3 6 100 Mass Non-mass 1 1 Invasive ductal carcinoma 10 17 18 20 Mass 7 3 7 3 Non-mass Invasive lobular carcinoma 2 8 9 9 Mass 1 1 Non-mass 1 1 Invasive medullary carcinoma 1 11 12 13 Mass Non-mass 1 1 Invasive cancer of non–special type 1 11 10 11 Mass 1 1 Non-mass Fibrocystic mastopathy 4 ( n = 3) 16 17 10 Mass 1 1 Non-mass 1 2 3 Microglandular adenosis 2 ( n = 1) 10 5 13 Mass Non-mass 1 1 1 1 Imaging diagnosis Lymph node or fibroadenoma 16 ( n = 13) 7 6 7 Mass 4 6 6 1 2 13 Non-mass Mastopathy 2 15 14 16 Mass Non-mass 2 2
ABVS, automated breast volume scanning; HHUS, handheld ultrasonography; MRI, magnetic resonance imaging.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Sensitivity, Specificity, Diagnostic Accuracy, Positive Predictive Value, and Negative Predictive Value for HHUS and ABVS
Sensitivity Specificity Diagnostic Accuracy PPV NPV HHUS 100.0% 83.3% 89.7% 78.9% 100.0% ABVS 93.3% 83.3% 87.2% 77.8% 95.2%
ABVS, automated breast volume scanning; HHUS, handheld ultrasonography.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 4
Rate of Malignancy
BI-RADS HHUS ABVS MRI 1 — — — 2 — — — 3 — 1 — 4a — — — 4b — 1 1 4c 2 3 2 5 13 10 12
ABVS, automated breast volume scanning; BI-RADS, Breast Imaging Reporting and Data System; DCIS, ductal carcinoma in situ; HHUS, handheld ultrasonography; MRI, magnetic resonance imaging.
The BI-RADS 3 in ABVS was the DCIS.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 5
Accordance in Describing the Localizations of the Most Suspicious/Largest Lesions
HHUS and MRI ( n = 34) ABVS and MRI ( n = 35) Same quadrant 31/34 (91.2%) 33/35 (94.3%) Different quadrants 3/34 (8.8%) 2/35 (5.7%)
ABVS, automated breast volume scanning; HHUS, handheld ultrasonography; MRI, magnetic resonance imaging.
Table 6
Size Assessment Made With HHUS and ABVS With Lesion Size in MRI as Reference
HHUS ( n = 34) ABVS ( n = 35) Accurate estimation 27 (79.4%) 28 (80.0%) Underestimation 5 (14.7%) 5 (14.3%) Overestimation 2 (5.9%) 2 (5.7%)
ABVS, automated breast volume scanning; HHUS, handheld ultrasonography; MRI, magnetic resonance imaging.
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgment
Get Radiology Tree app to read full this article<
References
1. Bick U.: Intensified surveillance for early detection of breast cancer in high-risk patients. Breast Care 2015; 10: pp. 13-20.
2. Smetherman D.H.: Screening, imaging, and image-guided biopsy techniques for breast cancer. Surg Clin North Am 2013; 93: pp. 309-327.
3. Demartini W.B., Eby P.R., Peacock S., et. al.: Utility of targeted sonography for breast lesions that were suspicious on MRI. AJR Am J Roentgenol 2009; 192: pp. 1128-1134.
4. Lu L.S., Chen L., Ding W.X., et. al.: Elevated expression of both MDR1 and MMP-2 genes in metastasized lymph node of invasive ductal breast cancer. Eur Rev Med Pharmacol Sci 2012; 16: pp. 2037-2043.
5. Tozaki M., Isobe S., Yamaguchi M., et. al.: Optimal scanning technique to cover the whole breast using an automated breast volume scanner. Jpn J Radiol 2010; 28: pp. 325-328.
6. Maturo V.G., Zusmer N.R., Gilson A.J., et. al.: Ultrasound of the whole breast utilizing a dedicated automated breast scanner. Radiology 1980; 137: pp. 457-463.
7. Arbeitsgemeinschaft Mammadiagnostik der Deutschen Röntgengesellschaft : Empfehlungen zur MR-Mammographie. Fortschr Röntgenstr 2005; 177: pp. 474-475.
8. Breast Imaging Working Group of the German Radiological Society: Updated Recommendations for MRI of the breast.2014. 186; 482–483
9. Wenkel E., Heckmann M., Heinrich M., et. al.: Automated breast ultrasound: lesion detection and BI-RADS classification—a pilot study. Rofo 2008; 180: pp. 804-808.
10. Kuhl C.: The current status of breast MR imaging. Part I. Choice of technique, image interpretation, diagnostic accuracy, and transfer to clinical practice. Radiology 2007; 244: pp. 356-378.
11. Abe H., Schmidt R.A., Shah R.N., et. al.: MR-directed (“Second-Look”) ultrasound examination for breast lesions detected initially on MRI: MR and sonographic findings. AJR Am J Roentgenol 2010; 194: pp. 370-377.
12. Vandromme M.J., Umphrey H., Kontrias H.: Image-guided methods for biopsy of suspicious breast lesions. J Surg Oncol 2011; 103: pp. 299-305.
13. Schueller G., Jaromi S., Ponhold L., et. al.: US-guided 14-gauge core-needle breast biopsy: results of a validation study in 1352 cases. Radiology 2008; 248: pp. 406-413.
14. La Trenta L.R., Menell J.H., Morris E.A., et. al.: Breast lesions detected with MR imaging: utility and histopathologic importance of identification with US. Radiology 2003; 227: pp. 856-861.
15. Wiratkapun C., Duke D., Nordmann A.S., et. al.: Indeterminate or suspicious breast lesions detected initially with MR imaging: value of MRI-directed breast ultrasound. Acad Radiol 2008; 15: pp. 618-625.
16. Wang Z.L., Xu J.H., Li J.L., et. al.: Comparison of automated breast volume scanning to hand-held ultrasound and mammography. Radiol Med 2012; 117: pp. 1287-1293.
17. Lin X., Wang J., Han F., et. al.: Analysis of eighty-one cases with breast lesions using automated breast volume scanner and comparison with handheld ultrasound. Eur J Radiol 2012; 81: pp. 873-878.
18. Wojcinski S., Farrokh A., Hille U., et. al.: The Automated Breast Volume Scanner (ABVS): initial experiences in lesion detection compared with conventional handheld B-mode ultrasound: a pilot study of 50 cases. Int J Womens Health 2011; 3: pp. 337-346.
19. Xiao Y.M., Chen Z.H., Zhou Q.C., et. al.: The efficacy of automated breast volume scanning over conventional ultrasonography among patients with breast lesions. Int J Gynaecol Obstet 2015; 131: pp. 293-296.
20. Li N., Jiang Y.-X., Zhu Q.-L., et. al.: Accuracy of an automated breast volume ultrasound system for assessment of the pre-operative extent of pure ductal carcinoma in situ: comparison with a conventional handheld ultrasound examination. Ultrasound Med Biol 2013; 39: pp. 2255-2263.
21. Zhang Q., Hu B., Hu B., et. al.: Detection of breast lesions using an automated breast volume scanner system. J Int Med Res 2012; 40: pp. 300-306.
22. Zheng F.Y., Yan L.X., Huang B.J., et. al.: Comparison of retraction phenomenon and BI-RADS-US descriptors in differentiating benign and malignant breast messes using an automated breast volume scanner. Eur J Radiol 2015; 84: pp. 2123-2129.
23. Jackson V.P., Kelly-Fry E., Rothschild P.A., et. al.: Automated breast sonography using a 7.5 MHz PVDF transducer: preliminary clinical evaluation. Work in progress. Radiology 1986; 159: pp. 679-684.
24. Cho K.R., Seo B.K., Lee J.Y., et. al.: A comparative study of 2D and 3D ultrasonography for evaluation of solid breast masses. Eur J Radiol 2005; 54: pp. 365-370.
25. Athanasiou A., Tardivon A., Ollivier L., et. al.: How to optimize breast ultrasound. Eur J Radiol 2009; 69: pp. 6-13.
26. Cho N., Moon W.K., Cha J.H., et. al.: Differentiating benign from malignant solid breast masses: comparison of two-dimensional and three-dimensional US. Radiology 2006; 240: pp. 26-32.
27. Zhang J., Lai X.J., Zhu Q.L., et. al.: Interobserver agreement for sonograms of breast lesions obtained by an automated breast volume scanner. Eur J Radiol 2012; 81: pp. 2179-2183.
28. Chou Y.H., Tiu C.M., Chen J., et. al.: Automated full-field breast ultrasonography: the past and the present. J Med Ultrasound 2007; 15: pp. 31-44.
29. Chae E.Y., Shin H.J., Kim H.J., et. al.: Diagnostic performance of automated breast ultrasound as a replacement for a hand-held second-look ultrasound for breast lesions detected initially on magnetic resonance imaging. Ultrasound Med Biol 2013; 39: pp. 2246-2254.
30. Chen L., Chen Y., Diao X.-H., et. al.: Comparative study of automated breast 3-D-ultrasound and handheld B-mode ultrasound for differentiation of benign and malignant breast masses. Ultrasound Med Biol 2013; 39: pp. 1735-1742.
31. Wang H.-Y., Jiang Y.-X., Zhu Q.-L., et. al.: Differentiation of benign and malignant breast lesions: a comparison between automatically generated breast volume scans and handheld ultrasound examinations. Eur J Radiol 2012; 81: pp. 3190-3200.
32. Buadu L.D., Murakami J., Murayama S., et. al.: Colour Doppler sonography of breast masses: a multiparameter analysis. Clin Radiol 1997; 52: pp. 917-923.
33. Jung H.J., Hahn S.Y., Choi H.Y., et. al.: Breast sonographic elastography using an advanced breast tissue-specific imaging preset: initial clinical results. J Ultrasound Med 2012; 31: pp. 273-280.
34. Arleo E.K., Saleh M., Ionescu D., et. al.: Recall rate of screening ultrasound with automated breast volume scanning (ABVS) in women with dense breasts: a first quarter experience. Clin Imaging 2014; 38: pp. 439-444.