
Rationale and Objectives
Perform a meta-analysis evaluating the diagnostic performance of magnetic resonance imaging (MRI) for the diagnosis of acute appendicitis.
Materials and Methods
MEDLINE and EMBASE were queried between January 1995 and December 2009. Prospective and retrospective studies were included if they: used MRI as a diagnostic test for appendicitis, used pathology or clinical follow-up as the reference standard, and reported absolute number of true-positive, true-negative, false-positive, and false-negative results, or stated sufficient data to derive these values. Summary sensitivity, summary specificity, positive and negative likelihood ratios (LR+) and (LR-), and diagnostic odds ratio were calculated. Heterogeneity of the results was assessed using Forest plots and the value of inconsistency index (I 2 ).
Results
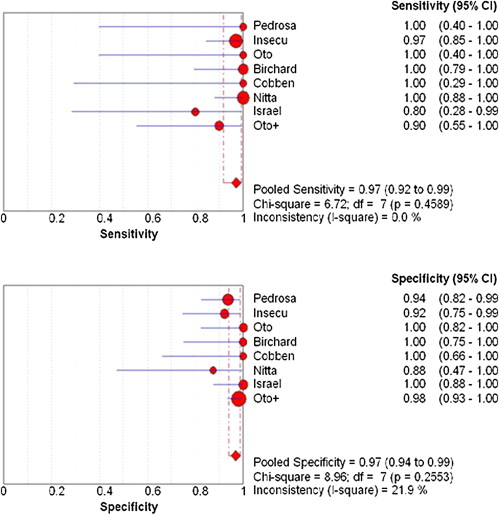
The inclusion criteria were fulfilled by eight articles with a total of 363 patients (mean age 26.9 ± 7.2 years; 86.2 % female). The appendix was not found in eight patients, with one article not reporting such data. The summary sensitivity was 97% (92%–99% at 95% confidence interval [CI]) and summary specificity was 95% (CI: 94%–99%), with a LR+ of 16.3 (CI: 9.1–29.1) and a LR- of 0.09 (CI: 0.04–0.197). Diagnostic odds ratio was 299.85 (CI: 97.5–921.61). No heterogeneity was found in the sensitivity (I 2 = 0.0, P = .4589). Minimal heterogeneity was found in the specificity (I 2 = 21.9%, P = .2553).
Conclusion
MRI appears promising in the evaluation of acute appendicitis, although larger future studies are warranted to confirm the results.
Acute appendicitis is a common etiology for acute abdominal pain and the need for emergent surgery. Although clinical and laboratory correlation may be enough for diagnosis, more clinicians are relying on radiological evaluation of the abdomen to make a definitive diagnosis . Additionally, up to one third of patients with appendicitis present with atypical symptoms that complicate a clinical diagnosis of appendicitis . Additionally, certain laboratory parameters may mire clinical diagnosis, such as physiologic leukocytosis of pregnancy . These dilemmas can potentially lead to unnecessary surgical intervention, thus more clinicians are using radiological evaluation for a definitive diagnosis .
Computed tomography (CT) is an established radiological procedure for the evaluation of acute appendicitis, but exposes the patient to ionizing radiation . With rising concerns of the public and medical communities with regard to increasing number of studies leading to increasing ionizing radiation exposure, alternative modalities have been investigated as potential diagnostic tools. This is especially true for pregnant patients, for whom acute appendicitis is the most common cause of acute abdomen and there are special considerations to avoid ionizing radiation. .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Execution of Data Collection and Statistical Analysis
Get Radiology Tree app to read full this article<
Data Sources and Searches
Get Radiology Tree app to read full this article<
Study Selection
Get Radiology Tree app to read full this article<
Data Extraction and Quality Assessment
Get Radiology Tree app to read full this article<
Data Synthesis and Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
LR+=sensitivity/(1−specificity) LR
+
=
sensitivity
/
(
1
-
specificity
)
LR−=(1−sensitivity)/specificity LR
-
=
(
1
-
sensitivity
)
/
specificity
A LR+ >10 and a LR- <0.1 implies a large and often conclusive increase or decrease in the likelihood of disease, respectively.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
dOR=LR+/LR− dOR
=
LR
+
/
LR
-
The dOR ranges from 0 to infinity. The higher the value, the better the test is at discriminating between those with and without the disease. A value of 1 is indicative of no discrimination. A value less than 1 indicates tests were interpreted poorly (more negative tests among those with disease).
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
I2=100[(Q−df)/Q] I
2
=
100
[
(
Q
-
df
)
/
Q
]
where Q is Cochran’s heterogeneity statistic and df is the degrees of freedom. A value of 0% indicates no heterogeneity and any value greater than 50% may be considered significant heterogeneity. Overall prevalence of appendicitis in the studies that met inclusion criterion was also calculated.
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Characteristics of Study Populations
First Author Journal (Year) Total Number of Patients ( n ) Number Female Mean Age (y) Scanner Brand and Strength (T) MRI Sequences Oto_Abdom. Imaging_ (2008) 118 118/118 26.9 General Electric (1.5) T2 FS; T2 SS FSE; STIR; T1 FSE; T1 GRE Cobben_Am J Roentgenol AJR_ (2004) 12 12/12 28 Siemens (1.0) T1 FLAS; T2 TSE; T2 TSE FS Incesu_Am J Roentgenol AJR_ (1997) 60 33/60 20 GE (0.5) T2 FSE, T1 SE; T2 FSE FS; T1 SE gad FS Birchard_Am J Roentgenol AJR_ (2005) 29 29/29 25 Siemens (1.5) T1 spoiled GRE; T2 HASTE; gad spoiled GRE Oto_Radiology_ (2005) 23 23/23 24.7 GE (1.5) T2 FSE; T2 FSE FS; STIR; T1 FSE Nitta_J. Magn. Reson. Imaging_ (2005) 27 14/27 37.1 Philips (0.5) T1 SE; T2 FSE; T2 FSE FS Pedrosa_Radiology_ (2006) 51 51/51 28.2 Siemens or GE (1.5) Oral ferumoxsil and barium sulfate for all; HF SS FSE; TOF T2 ∗ GRE; T1 IP/OP Israel_J. Magn. Reson. Imaging_ (2008) 33 33/33 25.6 GE (1.5) SS FSE; T2 FSE FS; T1
TSE, turbo spin echo; UTSE, ultra turbo spin echo; STIR, short tau inversion recovery; FLAS, fast low angle shot; FS, fat suppressed; gad, gadolinium enhanced; GRE, gradient recall echo; SS, single shot; TOF, time of flight; IP/OP, in phase/opposed phase; SE, spin echo; HF, half Fourier; HASTE, half Fourier single shot turbo spin echo; T, Tesla.
Table 2
Quality Assessment
First Author Item 1 Item 2 Item 3 Item 4 Item 5 Item 6 Item 7 Item 8 Item 9 Item 10 Score Oto ∗ Yes Yes Yes Yes No Yes Yes Yes Yes Yes 9 Cobben Yes No Yes No Yes Yes Yes Yes No Yes 7 Incesu Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes 10 Birchard Yes Yes No No Yes Yes Yes Yes No Yes 7 Oto Yes Yes Yes No No Yes Yes Yes No Yes 7 Nitta Yes Yes No No No Yes Yes No Yes Yes 6 Pedrosa Yes Yes Yes Yes No Yes Yes Yes Yes Yes 9 Israel Yes Yes No No No Yes Yes Yes No Yes 6
Item 1: Was the population clinically relevant, defined as a group of patients covering the spectrum of disease that is likely to be encountered in the current or future use of the test? Item 2: was there complete verification by the reference standard? Item 3: Was there blinded interpretation of the test results? Item 4: Was there consecutive patient selection? Item 5: Was there prospective enrollment of patients? Item 6: Was there adequate description and quality of the imaging procedure? Item 7: Was the quality of the reference test technically adequate? Item 8: Was there adequate clinical description of the patient population? Item 9: Was the sample size ≥35 patients? Item 10: Was there adequate reporting of results, including summary and subgrouping indexes of accuracy?
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Table 3
The Results from recent Meta-analyses in Diagnosing Acute Appendicitis using Magnetic Resonance Imaging, Computed Tomography, and/or Ultrasound
Authors Barger et al Doria et al ∗ van Randen et al Modality Magnetic resonance imaging Ultrasound Computed tomography Ultrasound Computed tomography Sensitivity 0.97 0.83 0.94 0.78 0.91 Specificity 0.97 0.93 0.94 0.83 0.90
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Birnbaum B.A., Wilson S.R.: Appendicitis at the millennium. Radiology 2000; 215: pp. 337-348.
2. Addiss D.G., Shaffer N., Fowler B.S., et. al.: The epidemiology of appendicitis in the United States. Am J Epidemiol 1990; 132: pp. 910-925.
3. Incesu L., Coskun A., Selcuk A.B., et. al.: Acute Appendicitis: MR imaging and sonographic correlation. Am J Roentgenol AJR 1997; 168: pp. 669-674.
4. Cappell M.S., Friedel D.: Abdominal pain during pregnancy. Gastroenterol Clin North Am 2003; 32: pp. 1-58.
5. Mourad J., Elliott J.P., Erickson L., et. al.: Appendicitis in pregnancy: new information that contradicts long-held clinical beliefs. Am J Obstet Gynecol 2000; 182: pp. 1027-1029.
6. Brown J.J.: Acute appendicitis: the radiologist’s role. Radiology 1991; 180: pp. 13-14.
7. Rosen M.P., Sands D.Z., Longmaid H.E., et. al.: Impact of abdominal CT on the management of patients presenting to the emergency department with acute abdominal pain. Am J Roentgenol AJR 2000; 174: pp. 1391-1396.
8. Terasawa T., Blackmore C.C., Bent S., et. al.: Systemic review: computed tomography and ultrasonography to detect acute appendicitis in adults and adolescents. Ann Intern Med 2004; 141: pp. 537-546.
9. Hormann M., Paya K., Eibenberger K., et. al.: MR imaging in children with nonperforated acute appendicitis: value of unenhanced MR imaging in sonographically selected cases. Am J Roentgenol AJR 1998; 171: pp. 467-470.
10. Andersen B., Nielsen T.F.: Appendicitis in pregnancy: diagnosis, management and complications. Acta Obstet Gynecol Scand 1999; 78: pp. 758-762.
11. Puylaert J.B.: Acute appendicitis: US evaluation using graded compression. Radiology 1986; 158: pp. 355-360.
12. Lim H.K., Bae S.H., Seo G.S.: Diagnosis of acute appendicitis in pregnant women: value of sonography. Am J Roentgenol 1992; 159: pp. 539-542.
13. Puylaert J.B.: Ultrasonography of the acute abdomen: gastrointestinal conditions. Radiol Clin North Am 2003; pp. 1227-1242. vii
14. Kessler N., Cyteval C., Gallix B., et. al.: Appendicitis: evaluation of sensitivity, specificity, and predictive values of US, Doppler US, and laboratory findings. Radiology 2004; 230: pp. 472-478.
15. Abu Yousef M.M., Bleicher J.J., Maher J.W., et. al.: High resolution sonography of acute appendicitis. Am J Roentgenol 1987; 149: pp. 53-58.
16. Sivit C.J., Newman K.D., Boenning D.A., et. al.: Appendicitis: usefulness of US in diagnosis in a pediatric population. Radiology 1992; 185: pp. 549-552.
17. Rioux M.: Sonographic detection of the normal and abnormal appendix. Am J Roentgenol 1992; 158: pp. 773-778.
18. Puylaert J.B., Rutgers P.H., Lalisang R.I., et. al.: A prospective study of ultrasonography in the diagnosis of appendicitis. N Engl J Med 1987; 317: pp. 666-669.
19. van Randen A., Bipat S., Zeinderman A.H., et. al.: Acute appendicitis: meta-analysis of diagnostic performance of CT and graded compression US related to prevalence of disease. Radiology 2008; 249: pp. 97-106.
20. Doria A.S., Moineddin R., Kellenberger C.J., et. al.: US or CT for diagnosis of appendicitis in children and adults? A meta-analysis. Radiology 2006; 241: pp. 83-94.
21. Oto A., Ernst R.D., Shah R., et. al.: Right-lower-quadrant pain and suspected appendicitis in pregnant women: evaluation with MR imaging-initial experience. Radiology 2005; 234: pp. 445-451.
22. Pedrosa I., Levine D., Eyvazzadeh A., et. al.: MR Imaging Evaluation of Acute Appendicitis in Pregnancy. Radiology 2006; 238: pp. 891-899.
23. Oto A, Ernst RD, Ghulmiyyah LM, et al. MR imaging in the triage of pregnant patients with acute abdominal pain. Available online at Abdom Imaging 2008; accessed January 5, 2009 at http://www.springerlink.com/content/cx637n43057q12u0 .
24. Israel G.M., Malguria N., McCarthy S., et. al.: MRI vs. Ultrasound for Suspected Appendicitis During Pregnancy. J Magn Resn Imaging 2008; 28: pp. 428-433.
25. Cobben L.P., Groot I., Haans L., et. al.: MRI for clinically suspected appendicitis during pregnancy. Am J Roengtenol AJR 2004; 183: pp. 671-675.
26. Birchard K.B., Brown M.A., Hyslop W.B., et. al.: MRI of acute abdominal pain and pelvic pain in pregnant patients. Am J Roentgenol AJR 2005; 184: pp. 452-458.
27. Nitta N., Takahashi M., Furukawa A., et. al.: MR imaging of the normal appendix and acute appendicitis. J Magn Res Imaging 2005; 21: pp. 156-185.
28. Whiting P., Rutjes A.W., Reitsma J.B., et. al.: The development of QUADAS: a tool for the quality of assessment of studies of diagnostic accuracy included in systematic reviews. BMC Med Res Methodol 2003; 3: Accessed on January 5, 2009, at http://www.biomedcentral.com/1471–2288/3/25
29. Zamora J., Abraira V., Muriel A., et. al.: Meta-DiSc: a software for meta-analysis of test accuracy data. BMC Med Res Meth 2006; 6: pp. 31.
30. Fischer J.E., Bachmann L.M., Jaeschke R.: A reader’s guide to the interpretation of diagnostic test properties: clinical example of sepsis. Intensive Care Med 2003; 29: pp. 1043-1051.
31. Glas A.S., Lijmer J.G., Prins M.H., et. al.: The diagnostic odds ratio: a single indicator of test performance. J Clin Epidemiol 2003; 56: pp. 1129-1135.
32. Singh A., Danrad R., Hahn P.F., et. al.: MR imaging of the acute abdomen and pelvis: acute appendicitis and beyond. Radiographics 2007; 27: pp. 1419-1431.
33. Lee K.S., Rofsky N.M., Pedrosa I.: Localization of the appendix at MR imaging during pregnancy: utility of the cecal tilt angle. Radiology 2008; pp. 249134-249141.