
Rationale and Objectives
For imaging pediatric appendicitis, ultrasonography (US) is preferred because of its lack of ionizing radiation, but is limited by operator dependence. This study investigates the US diagnostic performance during night shifts covered by radiology trainees compared to day shifts covered by attending radiologists.
Materials and Methods
Appy-Scores (1 = completely visualized normal appendix; 2 = partially visualized normal appendix; 3 = nonvisualized appendix with no inflammatory changes in the expected region of the appendix; 4 = equivocal; 5a = nonperforated appendicitis; 5b = perforated appendicitis) from 2935 US examinations (2161:774, day-to-night) from July 2013 to 2014 were correlated with the intraoperative diagnoses and the clinical follow-up. The diagnostic performance of trainees and attendings was compared with Fisher exact test. Interobserver agreement was measured by Cohen kappa coefficient.
Results
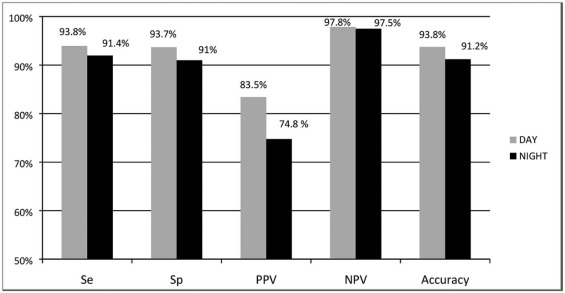
Appendicitis prevalence was 25.3% (day) and 22.5% (night). Sensitivity, specificity, accuracy, negative predictive value, and positive predictive vale were 94.0%, 93.7%, 93.8%, 97.9%, and 83.4% during the day and 92.0%, 91.2%, 91.3%, 97.5%, and 75.2% at night. Specificity ( P = .048) and positive predictive value ( P = .011) differed, with more false positives at night (7%) than during the day (4.7%). Trainee and attending agreement was high (k = 0.995), with Appy-Scores of 1, 4, and 5a most frequently discordant.
Conclusions
US has a high diagnostic performance and interobserver agreement for pediatric appendicitis when interpreted by radiology trainees during night shifts or attending radiologists during day shifts. However, lower specificity and positive predictive value at night warrants a thorough trainee education to avoid false-positive examinations.
Introduction
Appendicitis is the most common cause of childhood abdominal pain requiring urgent surgery and is the ultimate diagnosis in one-third of children admitted for abdominal pain . Ultrasonography (US) is the preferred imaging modality for evaluating suspected pediatric appendicitis because it is highly efficacious, noninvasive, and lacks ionizing radiation. However, a primary limitation of US is its high operator dependence . The visualization of the pediatric appendix by US and the diagnostic performance of US for pediatric appendicitis is greater when peformed by pediatric sonographers and interpreted by pediatric radiologists compared to adult specialists. The pediatric experience of technologists and radiologists may vary between day and night shifts depending on institutional staffing resources, resulting in variation of diagnostic performance between these shifts .
A wide variation of discrepancy rates (3%–30%) has been reported between on-call radiology trainee preliminary reports and faculty radiologist final interpretations . Clinically significant “major” discrepancies occur at an overall rate of around 1%, and are more common with cross-sectional imaging than with radiography . To our knowledge, the discrepancy rate between trainee and faculty radiologists has not been established in the setting of US for suspected pediatric appendicitis. Given the primary role of US in the diagnosis of pediatric appendicitis and the high operator dependence of US, we designed our study to compare the diagnostic performance of US examinations obtained for suspected pediatric appendicitis during night shifts (11 pm –7 am ) initially interpreted by radiology trainees without a faculty pediatric radiologist on site compared to day shifts (7 am –11 pm ) with a faculty radiologist present on site at the point of care. We hypothesized that a discrepancy in one or more diagnostic performance characteristics of US for pediatric appendicitis could be discerned between trainee and faculty radiologists. Identification of the nature of the discrepancy is important to better target further educational efforts and improve timely diagnosis of the most common pediatric abdominal surgical emergency.
Materials and Methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Distribution of Appy-Scores during Day and Night Relative to Final Diagnosis.
Appendicitis No Appendicitis TotalDAY Score 1 6 0.66% 903 99.34% 909 Score 2 2 1.34% 147 98.65% 149 Score 3 26 5.31% 464 94.69% 490 Score 4 26 23.01% 87 76.99% 113 Score 5a 392 97.03% 12 2.97% 404 Score 5b 94 97.92% 2 2.08% 96NIGHT Score 1 1 0.34% 291 99.66% 292 Score 2 2 4.88% 39 95.12% 41 Score 3 11 4.85% 216 95.15% 227 Score 4 8 15.09% 45 84.91% 53 Score 5a 124 94.66% 7 5.34% 131 Score 5b 28 93.33% 2 6.67% 30TOTAL 628 2307 2935
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Linam E.L., Munden M.: Sonography as the first line of evaluation in children with suspected acute appendicitis. J Ultrasound Med 2012; 31: pp. 1153-1157.
2. Addiss D.G., Shaffer N., Fowler B.S., et. al.: The epidemiology of appendicitis and appendectomy in the United States. Am J Epidemiol 1990; 132: pp. 910-925.
3. Pohl D., Golub R., Schwartz G.E., et. al.: Appendiceal ultrasonography performed by nonradiologists: does it help in the diagnostic process?. J Ultrasound Med 1998; 17: pp. 217-221.
4. Zielke A., Sitter H., Rampp T., et. al.: Clinical decision-making, ultrasonography, and scores for evaluation of suspected acute appendicitis. World J Surg 2001; 25: pp. 578-584.
5. Trout A.T., Sanchez R., Ladino-Torres M.F., et. al.: A critical evaluation of US for the diagnosis of pediatric acute appendicitis in a real-life setting: how can we improve the diagnostic value of sonography. Pediatr Radiol 2012; 42: pp. 813-823.
6. Stevens K.J., Griffiths K.L., Rosenberg J., et. al.: Discordance rates between preliminary and final radiology reports on cross-sectional imaging studies at a Level 1 trauma center. Acad Radiol 2008; 15: pp. 1217-1226.
7. Cooper V.F., Goodhartz L.A., Nemcek A.A., et. al.: Radiology resident interpretation of on-call imaging studies: the incidence of major discrepancies. Acad Radiol 2008; 15: pp. 1198-1204.
8. Ruutiainen A.T., Scanlon M.H., Itri J.N.: Identifying benchmarks for discrepancy rates in preliminary interpretations provided by radiology trainees at an academic institution. J Am Coll Radiol 2011; 8: pp. 644-648.
9. Fallon S.C., Orth R.C., Guillerman R.P., et. al.: Development and validation of an ultrasound scoring system for children with suspected acute appendicitis. Pediatr Radiol 2015; 45: pp. 1945-1952.
10. Fallon S.C., Kim M.E., Hallmark C.A., et. al.: Correlating surgical and pathological diagnoses in pediatric appendicitis. J Pediatr Surg 2015; 50: pp. 638-641.
11. Coyne S.M., Zhang B., Trout A.T.: Does appendiceal diameter change with age? A sonographic study. AJR Am J Roentgenol 2014; 203: pp. 936-945.
12. Goldin A.B., Khanna P., Thapa M., et. al.: Revised ultrasound criteria for appendicitis in children improve diagnostic accuracy. Pediatr Radiol 2011; 41: pp. 993-999.
13. Prendergast P.M., Poonai N., Lynch T., et. al.: Acute appendicitis: investigating an optimal outer appendiceal diameter cut-point in a pediatric population. J Emerg Med 2014; 46: pp. 157-164.
14. Huntley J.H., Carone M., Yousem D.M., et. al.: Opportunities for targeted education: critical neuroradiologic findings missed or misinterpreted by residents and fellows. AJR Am J Roentgenol 2015; 205: pp. 1155-1159.
15. McGlynn E.A., McDonald K.M., Cassel C.K.: Measurement is essential for improving diagnosis and reducing diagnostic error. A report from the Institute of Medicine. JAMA 2015; 314: pp. 2501-2502.
16. Ruutianinen A.T., Scanlon M.H., Itri J.N.: Identifying benchmarks for discrepancy rates in preliminary interpretations provided by radiology trainees at an academic institution. J Am Coll Radiol 2011; 8: pp. 644-648.