
Rationale and Objectives
The objective of this study was to assess the diagnostic utility of 3-tesla (3T) magnetic resonance imaging (MRI) of lungs in the detection of interstitial lung disease (ILD) in pediatric patients.
Materials and Methods
Twelve children (mean: 8.5 years, range: 4–12 years) with ILD were consecutively enrolled in this prospective study. HRCT and 3T lung MRI were performed in all patients within 2 days of each other. The sensitivity, the specificity, the positive predictive value, and the negative predictive value of detecting lung abnormalities related to ILD with 3T lung MRI were calculated, with high-resolution computed tomography (HRCT) as a standard of reference. Agreement between HRCT and 3T lung MRI, as well as between two reviewers, was calculated with the kappa coefficient.
Results
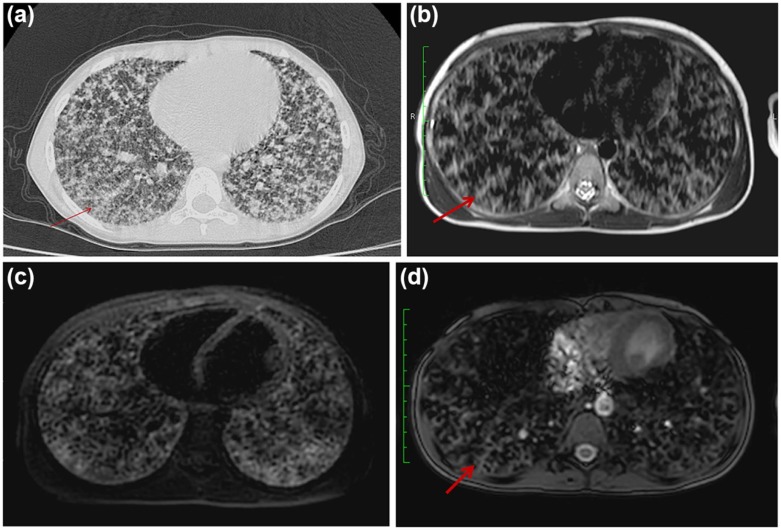
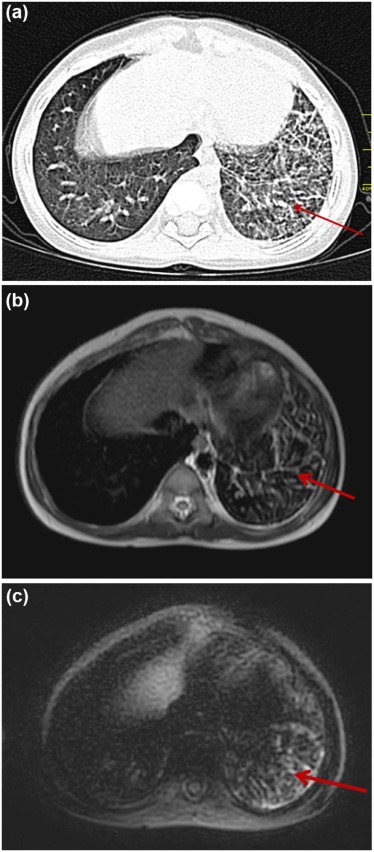
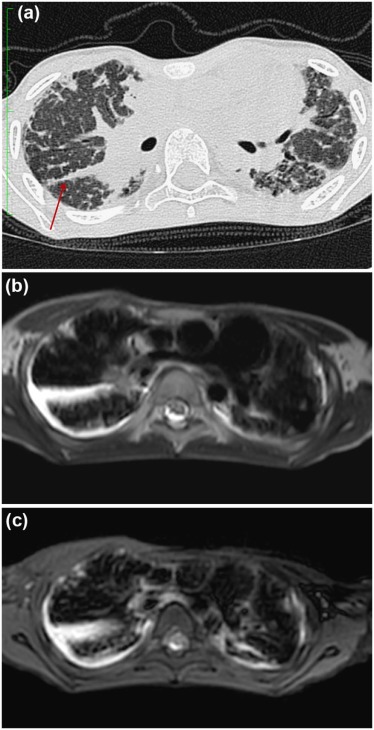
3T lung MRI had low sensitivity (66.67%) and high specificity (97.33%) in the detection of abnormalities related to ILD when compared to HRCT in children. Although 3T lung MRI performed well in the detection of consolidation, parenchymal bands and fissural thickening with a sensitivity of 100%, the sensitivity of 3T lung MRI in the detection of septal thickening, ground-glass opacity, nodules, and cysts was relatively low (50.0%, 50.0%, 66.67%, and 25.0%, respectively). Substantial agreement was seen between HRCT and 3T lung MRI ( k = 0.7), whereas perfect agreement was seen between two reviewers in detecting abnormalities related to pediatric ILD ( k = 0.9–1.0).
Conclusions
In comparison to HRCT, 3T lung MRI with routinely available MRI protocols and sequences can also well detect abnormalities such as consolidation, parenchymal bands, and fissural thickening in children with ILD. However, evaluation of septal thickening, ground-glass opacity, nodules, and cysts is limited with 3T lung MRI.
Introduction
Interstitial lung diseases (ILDs) in pediatric populations are a heterogeneous group of disorders with diffuse lung involvement, frequently leading to significant mortality and morbidity . Unlike the adult population, the spectrum of ILD in children is entirely different, with certain diseases unique to the pediatric population . In addition, clinical manifestations of ILD in children are unfortunately nonspecific and variable, often leading to missed or delayed diagnosis.
Main investigations employed for the diagnosis of ILD include imaging, pulmonary function tests, bronchoalveolar lavage, and lung biopsy. Pulmonary function tests are difficult to perform in children because of poor cooperation , and bronchoalveolar lavage is of diagnostic value in a substantially limited number of conditions . Tissue biopsy provides a definitive diagnosis but has disadvantage of being invasive. Considering the limitations of all these currently available investigations, imaging plays a crucial role in the diagnosis and evaluation of pediatric ILD.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and Methods
Get Radiology Tree app to read full this article<
Study Population
Get Radiology Tree app to read full this article<
Imaging Technique
HRCT Protocol
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
MRI Protocol
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
HRCT and MR Image Evaluation
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Diagnostic Criteria
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Study Cohort
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
HRCT Findings
Get Radiology Tree app to read full this article<
Table 1
HRCT and MRI Findings in Pediatric Patients with Interstitial Lung Disease
Imaging Findings Number and Percentage of Patients on HRCT Number and Percentage of Patients on MRI Consolidation 4/12 (33%) 4/12 (33%) Ground-glass opacity 2/12 (17%) 2/12 (17%) Nodules 3/12 (25%) 2/12 (17%) Cyst 4/12 (33%) 1/12 (8%) Septal thickening 4/12 (33%) 2/12 (17%) Bronchiectasis 0/12 (0%) 1/12 (8%) Parenchymal bands 2/12 (17%) 2/12 (17%) Fissural thickening 2/12 (17%) 2/12 (17%)
HRCT, high-resolution computed tomography; MRI, magnetic resonance imaging.
Get Radiology Tree app to read full this article<
MRI Findings
Get Radiology Tree app to read full this article<
Diagnostic Performance of MRI
Get Radiology Tree app to read full this article<
Table 2
Sensitivity, Specificity, PPV, and NPV of Magnetic Resonance Imaging in Detecting Lung Abnormalities in Pediatric Patients with Interstitial Lung Disease
Imaging Finding Sensitivity (%) Specificity (%) PPV (%) NPV (%) Consolidation 100 100 100 100 Parenchymal bands 100 100 100 100 Fissural thickening 100 100 100 100 Nodules 66.7 100 100 90 Ground-glass opacity 50 90 50 90 Septal thickening 50 100 100 80 Cyst 25 100 100 73 Bronchiectasis 0 92 0 100
NPV, negative predictive value; PPV, positive predictive value.
Get Radiology Tree app to read full this article<
Agreement Between HRCT and MRI
Get Radiology Tree app to read full this article<
Table 3
Agreement Between CT and MRI
Finding Agreement Between CT and MRI (kappa) Septal thickening .571 Bronchiectasis 0 Cyst .308 Parenchymal bands 1.00 Consolidation 1.00 Fissural thickening 1.00 Nodule .75 Ground-glass opacity .40
CT, computed tomography; MRI, magnetic resonance imaging.
Get Radiology Tree app to read full this article<
Agreement Between Two Reviewers
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgment
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Dinwiddie R., Sharief N., Crawford O.: Idiopathic interstitial pneumonitis in children: a national survey in the United Kingdom and Ireland. Pediatr Pulmonol 2002; 34: pp. 23-29.
2. Fan L.L., Kozinetz C.A.: Factors influencing survival in children with chronic interstitial lung disease. Am J Respir Crit Care Med 1997; 156: pp. 939-942.
3. Langston C., Fan L.L.: Diffuse interstitial lung disease in infants. Pediatr Pulmonol 2001; S23: pp. 74-76.
4. Clement A., Nathan N., Epaud R., et. al.: Interstitial lung diseases in children. Orphanet J Rare Dis 2010; 5: pp. 22.
5. deBlic J., Midulla F., Barbato A., et. al.: Bronchoalveolar lavage in children. ERS task force on bronchoalveolar lavage in children. European Respiratory Society. Eur Respir J 2000; 15: pp. 217-231.
6. Refabert L., Rambaud C., Mamou-Mani T., et. al.: Cd1a-positivecells in bronchoalveolar lavage samples from children with Langerhans cell histiocytosis. J Pediatr 1996; 129: pp. 913-915.
7. Midulla F., Strappini P.M., Ascoli V., et. al.: Bronchoalveolar lavage cell analysis in a child with chronic lipid pneumonia. EurRespir J 1998; 11: pp. 239-242.
8. Oermann C.M., Panesar K.S., Langston C., et. al.: Pulmonary infiltrates with eosinophilia syndromes in children. J Pediatr 2000; 136: pp. 351-358.
9. Copley S.J., Bush A.: HRCT of paediatric lung disease. PaediatrRespir Rev 2000; 1: pp. 141-147.
10. Klusmann M., Owens C.: HRCT in paediatric diffuse interstitial lung disease–a review for 2009. Pediatr Radiol 2009; 39: pp. 471-481.
11. Vrielynck S., Mamou-Mani T., Emond S., et. al.: Diagnostic value of high-resolution CT in the evaluation of chronic infiltrative lung disease in children. AJR Am J Roentgenol 2008; 191: pp. 914-920.
12. Rupprecht T., Böwing B., Kuth R., et. al.: Steady-state free precession projection MRI as a potential alternative to the conventional chest X-ray in pediatric patients with suspected pneumonia. Eur Radiol 2002; 12: pp. 2752-2756.
13. Yikilmaz A., Koc A., Coskun A., et. al.: Evaluation of pneumonia in children: comparison of MRI with fast imaging sequences at 1.5T with chest radiographs. Acta Radiol 2011; 52: pp. 914-919.
14. Abolmaali N.D., Schmitt J., Krauss S., et. al.: MR imaging of lung parenchyma at 0.2 T: evaluation of imaging techniques, comparative study with chest radiography and interobserver analysis. Eur Radiol 2004; 14: pp. 703-708.
15. Sodhi K.S., Khandelwal N., Saxena A.K., et. al.: Rapid lung MRI in children with pulmonary infections: time to change our diagnostic algorithms. J Magn Reson Imaging 2016; 43: pp. 1196-1206.
16. Sodhi K.S., Khandelwal N., Saxena A.K., et. al.: Rapid lung MRI: paradigm shift in evaluation of febrile neutropenia in children with leukemia: a pilot study. Leuk Lymphoma 2016; 57: pp. 70-75.
17. Lutterbey G., Grohé C., Gieseke J., et. al.: Initial experience with lung-MRI at 3.0 T: comparison with CT and clinical data in the evaluation of interstitial lung disease activity. Eur J Radiol 2007; 61: pp. 256-261.
18. Lutterbey G., Gieseke J., Von Falkenhausen M., et. al.: Lung MRI at 3.0 T: a comparison of helical CT and high-field MRI in the detection of diffuse lung disease. Eur Radiol 2005; 15: pp. 324-328.
19. Hansell D.M., Bankier A.A., MacMahon H., et. al.: Fleischner Society: glossary of terms for thoracic imaging 1. Radiology 2008; 246: pp. 697-722.
20. Eichinger M., Optazaite D.E., Kopp-Schneider A., et. al.: Morphologic and functional scoring of cystic fibrosis lung disease using MRI. Eur J Radiol 2012; 81: pp. 1321-1329.
21. Gorkem S.B., Köse S., Lee E.Y., et. al.: Thoracic MRI evaluation of sarcoidosis in children. Pediatr Pulmonol 2017; 52: pp. 494-499.
22. Chung J.H., Little B.P., Forssen A.V., et. al.: Proton MRI in the evaluation of pulmonary sarcoidosis: comparison to chest CT. Eur J Radiol 2013; 82: pp. 2378-2385.
23. Mirsadraee S., Tse M., Kershaw L., et. al.: T1 characteristics of interstitial pulmonary fibrosis on 3T MRI—a predictor of early interstitial change?. Quant Imaging Med Surg 2016; 6: pp. 42-49.
24. Müller C.S., Warszawiak D., Paiva E.D., et. al.: Pulmonary magnetic resonance imaging is similar to chest tomography in detecting inflammation in patients with systemic sclerosis. Rev Bras Reumatol 2017; 57: pp. 419-424.
25. Barreto M.M., Rafful P.P., Rodrigues R.S., et. al.: Correlation between computed tomographic and magnetic resonance imaging findings of parenchymal lung diseases. Eur J Radiol 2013; 82: pp. e492-e501.
26. Sodhi K.S., Krishna S., Saxena A.K., et. al.: Clinical application of “Justification” and “Optimization” principle of ALARA in pediatric CT imaging: “how many children can be protected from unnecessary radiation?”. Eur J Radiol 2015; 84: pp. 1752-1757.
27. Sodhi K.S., Lee E.Y.: What all physicians should know about the potential radiation risk that computed tomography poses for paediatric patients. Acta Paediatr 2014; 103: pp. 807-811.
28. Sodhi K.S., Khandelwal N.: Magnetic resonance imaging of lungs as a radiation-free technique for lung pathologies immunodeficient patients. J ClinImmunol 2016; 36: pp. 621-623.
29. Liszewski M.C., Ciet P., Sodhi K.S., et. al.: Updates on MRI evaluation of pediatric large airways. AJR Am J Roentgenol 2017; pp. 1-11. [Epub ahead of print]
30. Garg M.K., Gupta P., Agarwal R., et. al.: MRI: a new paradigm in imaging evaluation of allergic bronchopulmonary aspergillosis?. Chest 2015; 147: pp. e58-e59.
31. Sodhi K.S., Sharma M., Saxena A.K., et. al.: MRI in thoracic tuberculosis in children. Indian J Pediatr 2017;
32. Sodhi K.S., Bhalla A.S., Mahomed N., et. al.: Imaging of thoracic tuberculosis in children: current and future directions. Pediatr Radiol 2017; 47: pp. 1260-1268.