
Rationale and Objectives
Few data were available regarding the underlying burden of specific plaque types with increasing ages. The aim of this study was to assess the relationship of coronary artery calcium (CAC) score with total coronary plaque burden and the difference of underlying coronary plaque composition across differing aging groups using 64-slice multidetector computed tomography.
Materials and Methods
Multidetector computed tomographic images of 781 consecutive patients were evaluated using a 15–coronary segment model. Segment involvement score (the total number of segments with any plaque), segment stenosis score (the sum of maximal stenosis score per segment), total plaque score (the sum of the plaque amount per segment), and plaque composition were measured to compare with total CAC scores stratified by age tertile (lowest [ n = 274], <55 years; middle [ n = 242], 55–65 years; highest [ n = 265], >65 years).
Results
The mean age of the study population was 59 ± 13 years (481 men [62%]). With increasing age, higher segment involvement scores, segment stenosis scores, and total plaque scores were noted. Plaque burden was correlated significantly with total CAC scores in all tertiles. The percentage of partially calcified ( P < .001) and calcified ( P < .001) plaque increased with age, and in the highest age tertile, 87% of plaque contained calcium (calcified or mixed), compared to only 63% in the younger patients ( P < .001). Those aged >65 years were highly unlikely to have isolated noncalcified plaque (in the setting of a calcium score of 0). Younger patients were 10 times more likely to have isolated noncalcified plaque ( P < .001).
Conclusions
The absence of CAC strongly excludes obstructive disease, and CAC predicts the presence of coronary atherosclerotic plaque. However, the absence of any CAC does not exclude the presence of coronary atherosclerotic plaque, especially in patients aged <55 years. Plaque composition shifted from noncalcified to calcified plaque with increasing age, which may affect the vulnerability of these lesions over time.
Assessment of coronary calcium is feasible and reproducible with the use of electron-beam computed tomography. More recently, it is easily quantified using multidetector computed tomographic (MDCT) imaging with well-standardized scores . Contrast-enhanced MDCT, noninvasively established to evaluate coronary artery stenosis, enables the identification of coronary plaque composition and plaque burden, with high spatial resolution as well .
Atherosclerotic plaque consists of a variety of amorphous materials, including fibrous debris, cholesterol, and matrix materials such as calcium, and is characterized by smooth muscle cell proliferation . Arterial calcium development is intimately associated with the development of atherosclerotic plaque as a part of coronary plaque . Although it has been reported that there is a strong correlation between coronary calcification and coronary atherosclerosis , coronary artery calcium (CAC) score may reflect only the portion of “calcified” plaque of coronary plaque burden. Moreover, several studies have reported nonobstructive disease or low rates of obstructive disease in patients without CAC and acute coronary events occurring in patients without CAC, most commonly in young smokers . Few data were available regarding the underlying burden of specific plaque types with increasing age. We hypothesized that CAC is correlated with total plaque better in an older population and that as plaque ages, more calcified plaque will be seen, significantly decreasing the noncalcified plaque.
Get Radiology Tree app to read full this article<
Methods
Study Population
Get Radiology Tree app to read full this article<
CAC and MDCT Image Acquisition and Postprocessing
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Measurement of CAC Score
Get Radiology Tree app to read full this article<
Measurement of Plaque Burden
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Characteristics of Study Population according to Age Tertile
Variable Lowest Tertile (<55 y) ( n = 274) Middle Tertile (55–65 y) ( n = 242) Highest Tertile (>65 y) ( n = 265)P Age (y) 46 ± 8 59 ± 3 72 ± 6 <.01 Men 177 (64.6%) 150 (62.0%) 154 (58.1%) .06 Body mass index (kg/m 2 ) 32.0 ± 6.6 30.5 ± 5.2 29.8 ± 5.3 .12 Family history of heart disease 143 (53.8%) 132 (56.4%) 143 (56.7%) .75 Smoking 64 (23.6%) 50 (21.1%) 40 (15.4%) .03 Diabetes 44 (16.2%) 43 (18.1%) 61 (23.3%) .11 Hyperlipidemia 129 (47.3%) 144 (60.3%) 162 (61.4%) <.01 Hypertension 103 (38.0%) 121 (50.6%) 151 (57.6%) <.01 Coronary artery calcium score 1.0 (0–4.0) 4.0 (1.0–9.0) 8.0 (3.0–14.0) <.001
Data are expressed as mean ± standard deviation, as number (percentage), or as median (interquartile range).
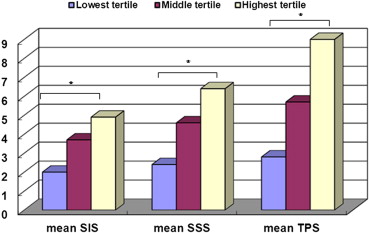
Table 2
Correlation Coefficient of Coronary Plaque Burden and Composition with Coronary Artery Calcium Scores in Each Age Tertile
Variable All ( n = 781) Lowest Tertile (<55 y) ( n = 274) Middle Tertile (55–65 y) ( n = 242) Highest Tertile (>65 y) ( n = 265) Segment involvement score 0.86 0.81 0.85 0.75 Noncalcified plaque † 0.09 0.27 −0.09 0.08 Partially calcified plaque ∗ 0.74 0.82 0.75 0.56 Calcified plaque ∗ 0.76 0.74 0.67 0.69 Segment stenosis score ∗ 0.87 0.80 0.88 0.80 Total plaque score ∗ 0.89 0.82 0.84 0.89
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
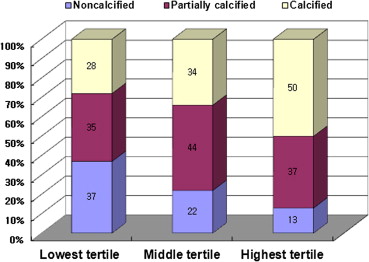
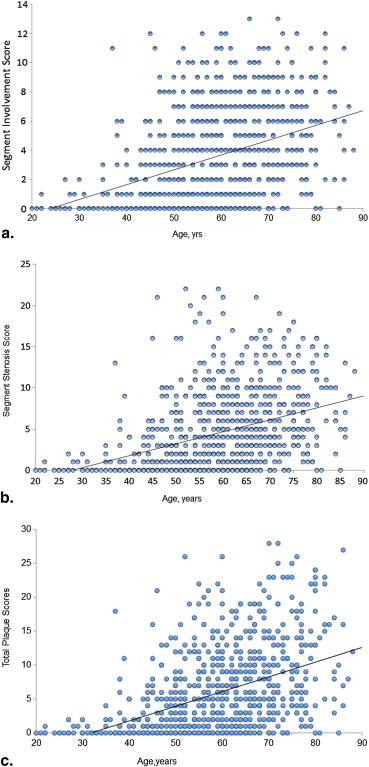
Table 3
Frequency of Plaque Subtypes among Age Tertiles
Variable Lowest Tertile ( n = 274) Middle Tertile ( n = 242) Highest Tertile ( n = 265)P No coronary plaque 108 (39.4%) 52 (21.5%) 29 (10.9%) <.001 Noncalcified plaque only 57 (20.8%) 15 (6.2%) 7 (2.6%) <.001 Partially calcified plaque only 12 (4.4%) 15 (6.2%) 14 (5.3%) <.001 Calcified plaque only 12 (4.4%) 19 (7.9%) 27 (10.2%) <.001 Combination of any plaque 83 (30.3%) 137 (56.6%) 186 (70.2%) <.001
Table 4
Odds Ratios (95% Confidence Intervals) for the Presence of Increasing Plaque Burden and Each Plaque Subtype according to Increasing Age in Multivariate-adjusted Analysis
Variable Lowest Tertile ( n = 274) Middle Tertile ( n = 242) Highest Tertile ( n = 265)P Plaque burden SIS 0 (referent) 1.6 (1.1 to 2.1) 2.8 (2.2 to 3.3) <.001 ∗ SSS 0 (referent) 2.1 (1.3 to 2.9) 3.8 (3.0 to 4.6) <.001 ∗ TPS 0 (referent) 2.7 (1.7 to 3.7) 5.8 (4.8 to 6.8) <.001 ∗ Plaque subtypes Noncalcified 0 (referent) 0.1 (−0.2 to 0.2) 0.1 (−0.3 to 0.1) .23 † Partially calcified 0 (referent) 0.9 (0.6 to 1.2) 1.1 (0.8 to 1.4) <.001 † Calcified 0 (referent) 0.7 (0.3 to 1.0) 1.8 (1.5 to 2.2) <.001 †
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 5
Odds Ratios (95% Confidence Intervals) for the Presence of More Than Three Segments with Plaque according to Increasing Ages in Multivariate-adjusted Analysis
More Than Three Segments with Plaque Lowest Tertile ( n = 274) Middle Tertile ( n = 242) Highest Tertile ( n = 265)P ∗ Noncalcified 1 (referent) 1.1 (0.8–1.6) 0.8 (0.6–1.1) .05 Partially calcified 1 (referent) 3.1 (2.0–4.8) 4.8 (3.1–7.2) <.001 Calcified 1 (referent) 2.8 (1.9–4.2) 8.1 (5.4–2.0) <.001
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Budoff M.J., Achenbach S., Blumenthal R.S., et. al.: Assessment of coronary artery disease by cardiac computed tomography: a scientific statement from the American Heart Association Committee on Cardiovascular Imaging and Intervention, Council on Cardiovascular Radiology and Intervention, and Committee on Cardiac Imaging, Council on Clinical Cardiology. Circulation 2006; 114: pp. 1761-1791.
2. Leber A.W., Becker A., Knez A., et. al.: Accuracy of 64-slice computed tomography to classify and quantify plaque volumes in the proximal coronary system: a comparative study using intravascular ultrasound. J Am Coll Cardiol 2006; 47: pp. 672-677.
3. Petranovic M., Soni A., Bezzera H., et. al.: Assessment of nonstenotic coronary lesions by 64-slice multidetector computed tomography in comparison to intravascular ultrasound: evaluation of nonculprit coronary lesions. J Cardiovasc Comput Tomogr 2009; 3: pp. 24-31.
4. Alexopoulos N., Raggi P.: Calcification in atherosclerosis. Nat Rev Cardiol 2009; 6: pp. 681-688.
5. Fitzpatrick L.A., Severson A., Edwards W.D., Ingram R.T.: Diffuse calcification in human coronary arteries. Association of osteopontin with atherosclerosis. J Clin Invest 1994; 94: pp. 1597-1604.
6. Bostrom K., Watson K.E., Horn S., et. al.: Bone morphogenetic protein expression in human atherosclerotic lesions. J Clin Invest 1993; 91: pp. 1800-1809.
7. Rumberger J.A., Simons D.B., Fitzpatrick L.A., et. al.: Coronary artery calcium area by electron-beam computed tomography and coronary atherosclerotic plaque area. A histopathologic correlative study. Circulation 1995; 92: pp. 2157-2162.
8. Sangiorgi G., Rumberger J.A., Severson A., et. al.: Arterial calcification and not lumen stenosis is highly correlated with atherosclerotic plaque burden in humans: a histologic study of 723 coronary artery segments using nondecalcifying methodology. J Am Coll Cardiol 1998; 31: pp. 126-133.
9. Cheng V.Y., Lepor N.E., Madyoon H., et. al.: Presence and severity of noncalcified coronary plaque on 64-slice computed tomographic coronary angiography in patients with zero and low coronary artery calcium. Am J Cardiol 2007; 99: pp. 1183-1186.
10. Rubinshtein R., Gaspar T., Halon D.A., et. al.: Prevalence and extent of obstructive coronary artery disease in patients with zero or low calcium score undergoing 64-slice cardiac multidetector computed tomography for evaluation of a chest pain syndrome. Am J Cardiol 2007; 99: pp. 472-475.
11. Schmermund A., Baumgart D., Gorge G., et. al.: Coronary artery calcium in acute coronary syndromes: a comparative study of electron-beam computed tomography, coronary angiography, and intracoronary ultrasound in survivors of acute myocardial infarction and unstable angina. Circulation 1997; 96: pp. 1461-1469.
12. Agatston A.S., Janowitz W.R., Hildner F.J., et. al.: Quantification of coronary artery calcium using ultrafast computed tomography. J Am Coll Cardiol 1990; 15: pp. 827-832.
13. Austen W.G., Edwards J.E., Frye R.L., et. al.: A reporting system on patients evaluated for coronary artery disease. Report of the Ad Hoc Committee for Grading of Coronary Artery Disease, Council on Cardiovascular Surgery, American Heart Association. Circulation 1975; 51: pp. 5-40.
14. Pagali S.R., Madaj P., Gupta M., et. al.: Interobserver variations of plaque severity score and segment stenosis score in coronary arteries using 64 slice multidetector computed tomography: a substudy of the ACCURACY trial. J Cardiovasc Comput Tomogr 2010; 4: pp. 312-318.
15. Detrano R., Hsiai T., Wang S., et. al.: Prognostic value of coronary calcification and angiographic stenoses in patients undergoing coronary angiography. J Am Coll Cardiol 1996; 27: pp. 285-290.
16. Frick M., Karakolcu F., Gschnitzer H., et. al.: Calcium score as assessed by multi-slice computed tomography does not predict maximum plaque burden: an in vitro study. Heart 2004; 90: pp. 1057-1058.
17. Bielak L.F., Rumberger J.A., Sheedy P.F., et. al.: Probabilistic model for prediction of angiographically defined obstructive coronary artery disease using electron beam computed tomography calcium score strata. Circulation 2000; 102: pp. 380-385.
18. Haberl R., Becker A., Leber A., et. al.: Correlation of coronary calcification and angiographically documented stenoses in patients with suspected coronary artery disease: results of 1,764 patients. J Am Coll Cardiol 2001; 37: pp. 451-457.
19. Budoff M.J., Diamond G.A., Raggi P., et. al.: Continuous probabilistic prediction of angiographically significant coronary artery disease using electron beam tomography. Circulation 2002; 105: pp. 1791-1796.
20. Knez A., Becker A., Leber A., et. al.: Relation of coronary calcium scores by electron beam tomography to obstructive disease in 2,115 symptomatic patients. Am J Cardiol 2004; 93: pp. 1150-1152.
21. Sarwar A., Shaw L.J., Shapiro M.D., et. al.: Diagnostic and prognostic value of absence of coronary artery calcification. JACC Cardiovasc Imaging 2009; 2: pp. 675-688.
22. Guerci A.D., Spadaro L.A., Popma J.J., et. al.: Relation of coronary calcium score by electron beam computed tomography to arteriographic findings in asymptomatic and symptomatic adults. Am J Cardiol 1997; 79: pp. 128-133.
23. Hoffmann U., Massaro J.M., Fox C.S., et. al.: Defining normal distributions of coronary artery calcium in women and men (from the Framingham Heart Study). Am J Cardiol 2008; 102: pp. 1136-1141.
24. Detrano R., Guerci A.D., Carr J.J., et. al.: Coronary calcium as a predictor of coronary events in four racial or ethnic groups. N Engl J Med 2008; 358: pp. 1336-1345.
25. Nakamura M., Nishikawa H., Mukai S., et. al.: Impact of coronary artery remodeling on clinical presentation of coronary artery disease: an intravascular ultrasound study. J Am Coll Cardiol 2001; 37: pp. 63-69.
26. Ehara S., Kobayashi Y., Yoshiyama M., et. al.: Spotty calcification typifies the culprit plaque in patients with acute myocardial infarction: an intravascular ultrasound study. Circulation 2004; 110: pp. 3424-3429.
27. Weiss R.M.: Another calcium paradox?. Arterioscler Thromb Vasc Biol 2001; 21: pp. 1561-1562.
28. Nasir K., Rivera J.J., Yoon Y.E., et. al.: Variation in atherosclerotic plaque composition according to increasing coronary artery calcium scores on computed tomography angiography. Int J Cardiovasc Imaging 2010; 26: pp. 923-932.
29. Lin F., Shaw L.J., Berman D.S., et. al.: Multidetector computed tomography coronary artery plaque predictors of stress-induced myocardial ischemia by SPECT. Atherosclerosis 2008; 197: pp. 700-709.
30. Pundziute G., Schuijf J.D., Jukema J.W., et. al.: Prognostic value of multislice computed tomography coronary angiography in patients with known or suspected coronary artery disease. J Am Coll Cardiol 2007; 49: pp. 62-70.
31. Cheng V.Y., Nakazato R., Dey D., et. al.: Reproducibility of coronary artery plaque volume and composition quantification by 64-detector row coronary computed tomographic angiography: an intraobserver, interobserver, and interscan variability study. J Cardiovasc Comput Tomogr 2009; 3: pp. 312-320.
32. Stary H.C., Chandler A.B., Dinsmore R.E., et. al.: A definition of advanced types of atherosclerotic lesions and a histological classification of atherosclerosis: a report from the Committee on Vascular Lesions of the Council on Arteriosclerosis, American Heart Association. Circulation 1995; 92: pp. 1355-1374.
33. Cho I., Chang H.J., Sung J.M., et. al., CONFIRM Investigators: Coronary computed tomographic angiography and risk of all-cause mortality and nonfatal myocardial infarction in subjects without chest pain syndrome from the CONFIRM registry (Coronary CT Angiography Evaluation for Clinical Outcomes: An International Multicenter Registry). Circulation 2012; 126: pp. 304-313.