
Rationale and Objectives
Although elevation of the diaphragm can be appreciated on conventional PA and lateral chest radiography, the modality is commonly viewed as inadequate to differentiate diaphragmatic paralysis from eventration. Our objective was to qualitatively and quantitatively measure the utility of chest radiography in determining the presence or absence of diaphragmatic paralysis in patients with an elevated diaphragm.
Materials and Methods
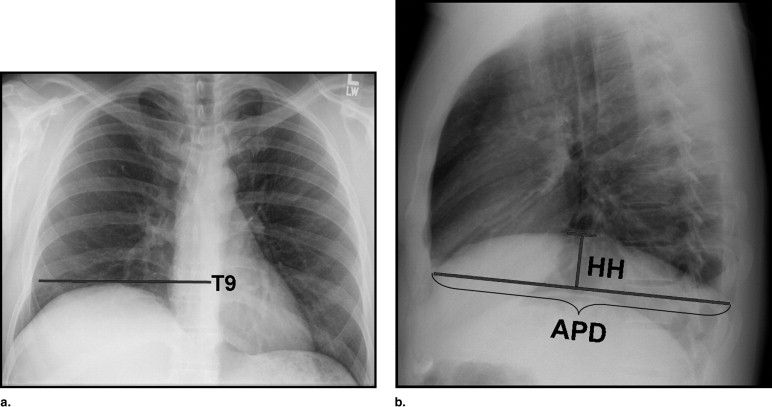
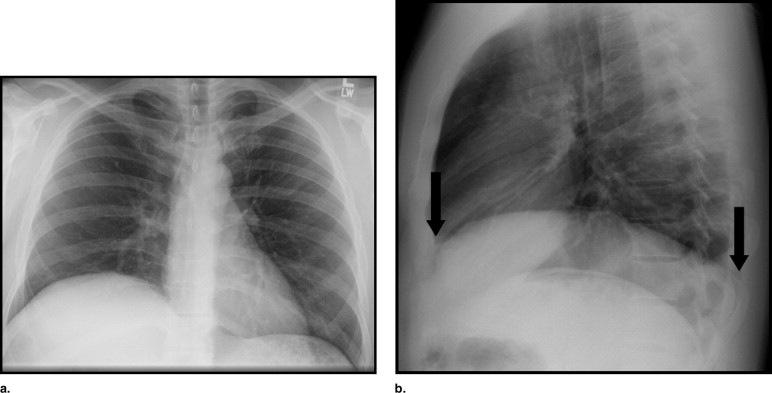
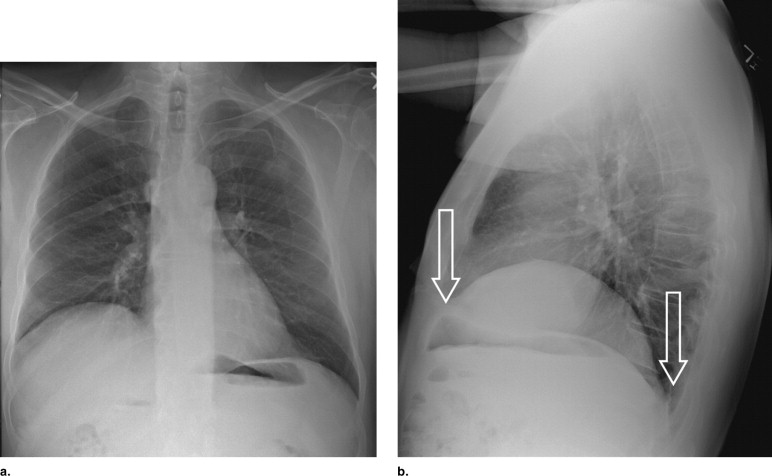
A retrospective analysis of chest radiographs in 32 patients, whom underwent fluoroscopic sniff test for elevated diaphragm, was performed. Diaphragm function was graded by a senior radiology resident, as either “paralyzed” or “non-paralyzed,” based on appearance/shape of elevated hemidiaphragm on PA and lateral radiograph. The diaphragm position and shape for all patients were determined using measurements relating to skeletal structures and radius of curvature, respectively. These results were correlated with the results of the fluoroscopic sniff tests.
Results
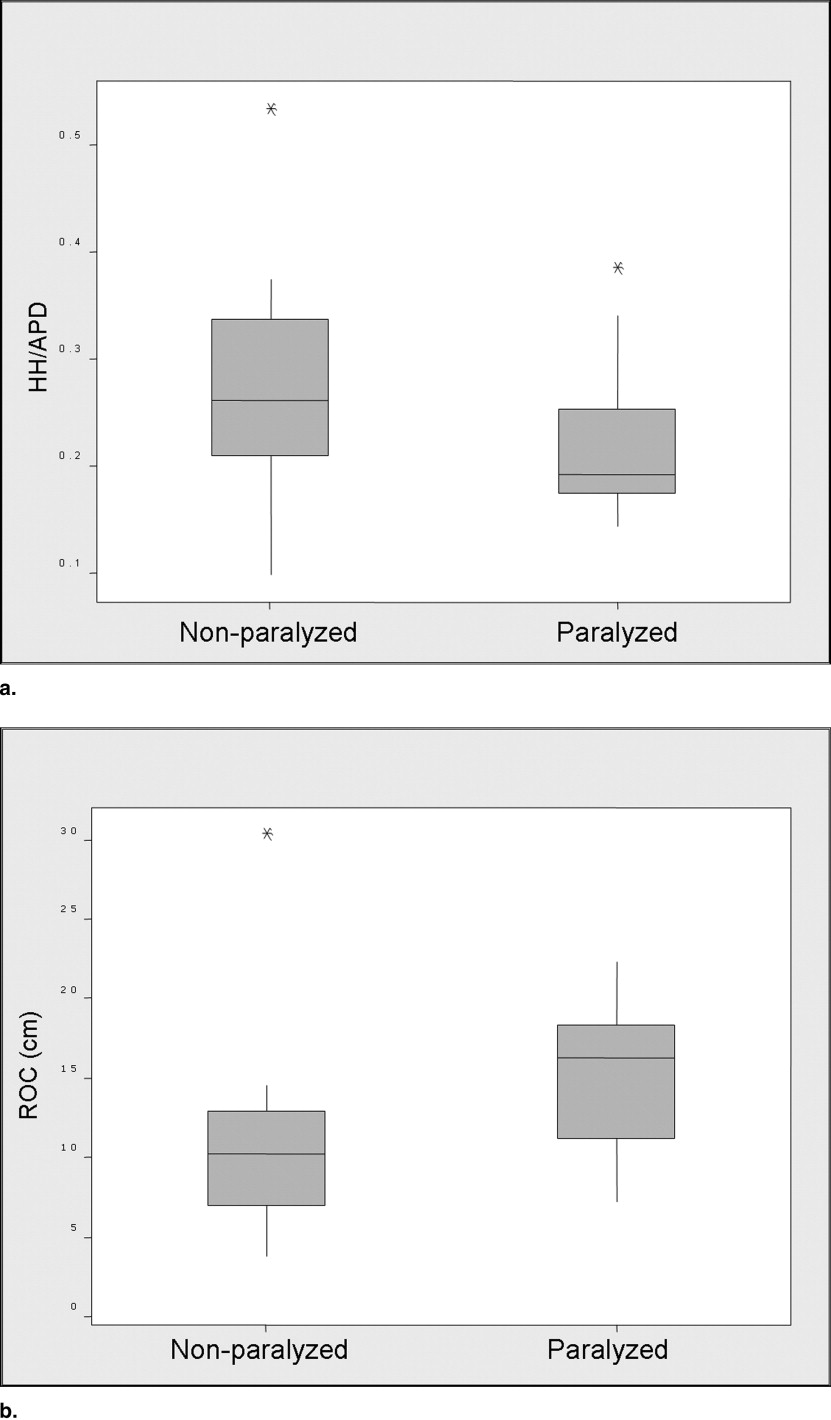
Of 32 patients with elevated diaphragm on chest radiograph, 17 had diaphragmatic paralysis confirmed with fluoroscopic sniff test. Our results indicate that the radius of curvature or shape of the diaphragm on lateral chest radiograph is the most important factor for detection of the presence or absence of diaphragmatic paralysis. HH/APD > 0.28 suggests against paralysis.
Conclusion
Conventional chest radiography appears to be a useful modality for assessment of the functional status of an elevated diaphragm. Based on our results, evaluation of the shape of an elevated diaphragm may preclude the need for fluoroscopic sniff test to determine diaphragmatic paralysis.
The diaphragm is a dome-shaped, fibromuscular partition between the thoracic and abdominal cavities, which provides most of the mechanical work of respiration. It is covered by pleura on the thoracic side and by peritoneum on the abdominal side and is in the extrapleural/extraperitoneal space. The diaphragm is peripherally composed of three groups of muscle fibers: 1) sternal portion (arises from back of xiphoid process), 2) costal portion (arising from lower six ribs and their costal cartilages), and 3) lumbar portion, which make up the crura (arising from medial and lateral arcuate ligaments and the lumbar vertebral bodies) and become the anterior longitudinal ligament of the spine. The central tendon of the diaphragm is a thin aponeurosis at the convergence of the muscular portions. Each hemidiaphragm is separately innervated by the right and left phrenic nerves and function independent of one another ( ). In most people, the right hemidiaphragm is 1.5 to 2.5 cm higher than the left, but the two hemidiaphragms are at the same level in about 9% of the population ( ).
Most diaphragmatic abnormalities are asymptomatic and are usually detected on a chest radiograph obtained for other reasons. The causes of diaphragmatic elevation are many and include pathology related directly to the diaphragm, as well as pathologic processes that indirectly cause diaphragm elevation ( ). The most common cause of apparent hemidiaphragm elevation is eventration, which describes a permanent elevation of all or portion of a hemidiaphragm with retention of its continuity and normal attachments to the costal margins. It is thought to be due to developmental abnormality of the diaphragm musculature ( ).
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Gibson G.J.: Diaphragmatic paresis: pathophysiology, clinical features, and investigation. Thorax 1989; 44: pp. 960-970.
2. Lennon E.A., Simon G.: The height of the diaphragm in the chest radiograph of normal adults. Brit J Radiol 1965; 38: pp. 937-943.
3. Wilcox P.G., Pardy R.L.: Diaphragmatic weakness and paralysis. Lung 1989; 167: pp. 323-341.
4. Deslauriers J.: Eventration of the diaphragm. Chest Surg Clin N Amer 1998; 8: pp. 315-330.
5. Gierada D.S., Slone R.M., Fleishman M.J.: Imaging evaluation of the diaphragm. Chest Surg Clin N Amer 1998; 8: pp. 237-280.
6. Tarver R.D., Conces D.J., Cory D.A., Vix V.A.: Imaging the diaphragm and its disorders. J Thorac Imaging 1989; 4: pp. 1-18.
7. Suwatanapongched T., Gierada D.S., Slone R.M., Pilgram T.K., et. al.: Variation in diaphragm position and shape in adults with normal pulmonary function. Chest 2003; 123: pp. 2019-2027.