
Rationale and Objectives
Cervical disc degeneration can result in nerve root compression and severe symptoms that significantly impair the patient’s quality of life. The purpose of this study is to investigate multiple diffusion metrics changes in the diffusion tensor imaging (DTI) of cervical nerve roots and their relationship with the clinical severity of patients with cervical disc herniation.
Materials and Methods
High directional DTI of the cervical nerve roots was performed in 18 symptomatic patients and 10 healthy volunteers with a 3.0-T magnetic resonance system after a routine cervical disc scanning. The fractional anisotropy (FA), mean diffusivity (MD), axial diffusivity (AD), and radial diffusivity (RD) were calculated from the DTI data and compared between the affected and unaffected sides in the same patient and between healthy volunteers and symptomatic patients. The correlation between the side-to-side diffusion metric differences and the clinical International Standards for Neurological Classification of Spinal Cord Injury scores was analyzed.
Results
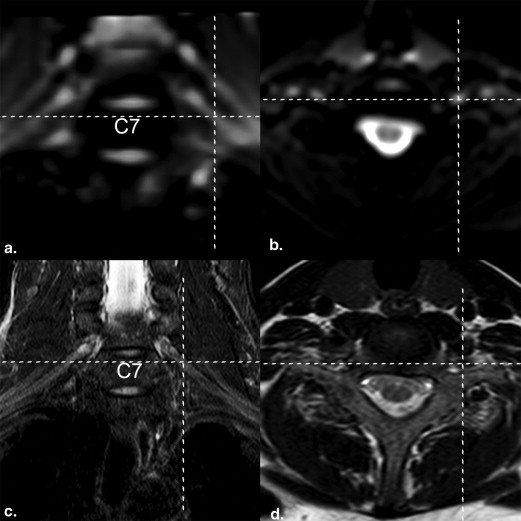
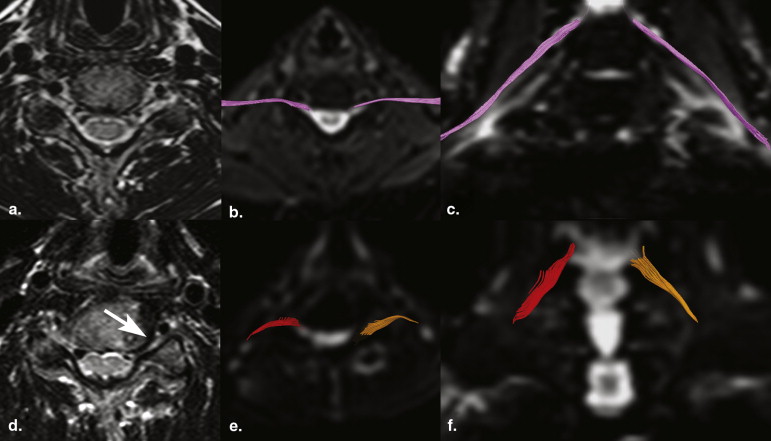
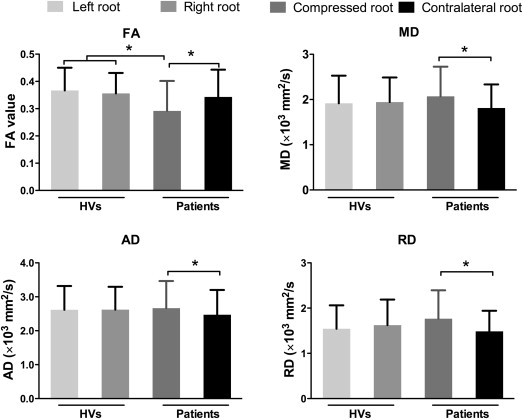
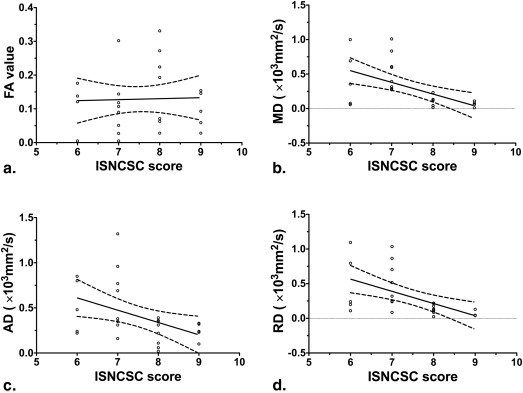
C5–C8 nerve roots were clearly delineated with DTI. The FA, MD, AD, and RD of compressed nerve roots were 0.31 ± 0.091, 2.06 ± 0.536, 2.69 ± 0.657, and 1.75 ± 0.510 mm 2 /s, respectively. Compared to the unaffected side or healthy volunteers, the nerve roots of the affected side showed decreased FA ( P < .022) and increased MD ( P < .035), AD ( P < .047), and RD ( P < .012). The clinical International Standards for Neurological Classification of Spinal Cord Injury scores of the patients were negatively correlated with MD ( r = −0.57, P = .002), AD ( r = −0.451, P = .021), and RD ( r = −0.564, P = .003) but not with FA ( r = 0.004, P = .984).
Conclusions
DTI can potentially be used to assess microstructural abnormalities in the cervical nerve roots in patients with disc herniation.
Diffusion tensor imaging (DTI) based on magnetic resonance (MR) imaging (MRI) can provide valuable information about tissue microstructure changes by applying a motion probing gradient in some directions for the in vivo monitoring of the potentially restricted, random microscopic motion of water molecules in tissues . The amount of nonrandom water diffusion that results from microstructural damage within diseased tissues can be quantified using DTI data . Diffusion tensor tractography (DTT), which is generated from the reconstruction and analysis of the data obtained by DTI, can be used to follow the orientation of nerve fibers and thereby trace specific neural pathways .
Previously, DTT has been widely applied in the central nerve system (i.e., brain and spinal cord) and less commonly in peripheral nerves such as the sciatic, median, radial, and ulnar nerves . The results of previous studies showed that DTI with fiber tracking might provide information and depict abnormalities beyond the resolution of conventional anatomic MR techniques. Quantitative DTI indices, such as the fractional anisotropy (FA) and apparent diffusion coefficient (ADC) values, have been reported to be abnormal in areas that may appear normal in structural MR images . Recently, DTT examination of the lumbar nerves or sacral plexus was successfully achieved in healthy volunteers (HVs) and patients with disc herniation . The results indicated that the compressed nerve roots have a decreased FA value and increased diffusivities, which may reflect microstructural changes of the compressed nerves in patients with disc herniation before conventional MRI. Comparatively, cervical disc degeneration can result in cervical nerve root compression early and can easily induce severe symptoms that significantly impair the quality of life of patients. However, as far as we know, the usefulness of DTI in evaluation of the compressed cervical nerve roots has not been investigated previously.
Get Radiology Tree app to read full this article<
Materials and methods
Subjects
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
MR Acquisition
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Data Processing and Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Ethical Aspects
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Fractional Anisotropy (FA), Mean Diffusivity (MD), Axial Diffusivity (AD), and Radial Diffusivity (RD) Measured in Healthy volunteers and Symptomatic Patients
Healthy Volunteers Patients Left Root Right Root Difference ∗ Compressed Root Contralateral Root Difference † FA 0.367 ± 0.083 0.356 ± 0.075 0.011 ± 0.058 0.292 ± 0.110 0.343 ± 0.100 −0.051 ± 0.160 ‡ MD ( × 10 3 mm 2 /sec) 1.916 ± 0.611 1.944 ± 0.544 0.028 ± 0.471 2.070 ± 0.655 1.813 ± 0.520 0.257 ± 0.340 ‡ AD ( × 10 3 mm 2 /sec) 2.620 ± 0.698 2.623 ± 0.673 0.003 ± 0.590 2.666 ± 0.800 2.470 ± 0.730 0.195 ± 0.478 ‡ RD ( × 10 3 mm 2 /sec) 1.543 ± 0.518 1.623 ± 0.565 0.080 ± 0.430 1.767 ± 0.628 1.484 ± 0.456 0.282 ± 0.339 ‡
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Basser P.J., Jones D.K.: Diffusion-tensor MRI: theory, experimental design and data analysis: a technical review. NMR Biomed 2002; 15: pp. 456-467.
2. Beaulieu C.: The basis of anisotropic water diffusion in the nervous system: a technical review. NMR Biomed 2002; 15: pp. 435-455.
3. Mori S., Zhang J.: Principles of diffusion tensor imaging and its applications to basic neuroscience research. Neuron 2006; 51: pp. 527-539.
4. Wiegell M.R., Larsson H.B., Wedeen V.J.: Fiber crossing in human brain depicted with diffusion tensor MR imaging. Radiology 2000; 217: pp. 897-903.
5. Bosma R., Stroman P.W.: Diffusion tensor imaging in the human spinal cord: development, limitations, and clinical applications. Crit Rev Biomed Eng 2012; 40: pp. 1-20.
6. Cauley K.A., Filippi C.G.: Diffusion-tensor imaging of small nerve bundles: cranial nerves, peripheral nerves, distal spinal cord, and lumbar nerve roots- clinical applications. AJR Am J Roentgenol 2013; 201: pp. W326-W335.
7. Vargas M.I., Delavelle J., Jlassi H., et. al.: Clinical applications of diffusion tensor tractography of the spinal cord. Neuroradiology 2008; 50: pp. 25-29.
8. Balbi V., Budzik J.F., Duhamel A., et. al.: Tractography of lumbar nerve roots: initial results. Eur Radiol 2011; 21: pp. 1153-1159.
9. Van der Jagt P.K., Dik P., Froeling M., et. al.: Architectural configuration and microstructural properties of the sacral plexus: a diffusion tensor MRI and fiber tractography study. Neuroimage 2012; 62: pp. 1792-1799.
10. Eguchi Y., Ohtori S., Orita S., et. al.: Quantitative evaluation and visualization of lumbar foraminal nerve root entrapment by using diffusion tensor imaging: preliminary results. Am J Neuroradiol 2011; 32: pp. 1824-1829.
11. Eguchi Y., Ohtori S., Yamashita M., et. al.: Clinical applications of diffusion magnetic resonance imaging of the lumbar foraminal nerve root entrapment. Eur Spine J 2010; 19: pp. 1874-1882.
12. Karampinos D.C., Melkus G., Shepherd T.M., et. al.: Diffusion tensor imaging and T2 relaxometry of bilateral lumbar nerve roots: feasibility of in-plane imaging. NMR Biomed 2013; 26: pp. 630-637.
13. American Spinal Injury Association. International Standards for Neurological Classification of Spinal Cord Injury, revised 2011. Atlanta, GA, 2011.
14. Sun S.W., Liang H.F., Le T.Q., et. al.: Differential sensitivity of in vivo and ex vivo diffusion tensor imaging to evolving optic nerve injury in mice with retinal ischemia. Neuroimage 2006; 32: pp. 1195-1204.
15. Eguchi Y., Ohtori S., Yamashita M., et. al.: Diffusion-weighted magnetic resonance imaging of symptomatic nerve root of patients with lumbar disc herniation. Neuroradiology 2011; 53: pp. 633-641.
16. Hiltunen J., Kirveskari E., Numminen J., et. al.: Pre- and post-operative diffusion tensor imaging of the median nerve in carpal tunnel syndrome. Eur Radiol 2012; 22: pp. 1310-1319.
17. Liu Y., Li J., Butzkueven H., et. al.: Microstructural abnormalities in the trigeminal nerves of patients with trigeminal neuralgia revealed by multiple diffusion metrics. Eur J Radiol 2013; 82: pp. 783-786.
18. Acosta-Cabronero J., Williams G.B., Pengas G., et. al.: Absolute diffusivities define the landscape of white matter degeneration in Alzheimer’s disease. Brain 2010; 133: pp. 529-539.
19. Liu Y., Duan Y., He Y., et. al.: A tract-based diffusion study of cerebral white matter in neuromyelitis optica reveals widespread pathological alterations. Mult Scler 2012; 18: pp. 1013-1021.
20. Khalil C., Hancart C., Le Thuc V., et. al.: Diffusion tensor imaging and tractography of the median nerve in carpal tunnel syndrome: preliminary results. Eur Radiol 2008; 18: pp. 2283-2291.
21. Andreisek G., White L.M., Kassner A., et. al.: Evaluation of diffusion tensor imaging and fiber tractography of the median nerve: preliminary results on intrasubject variability and precision of measurements. AJR Am J Roentgenol 2010; 194: pp. W65-W72.
22. Guggenberger R., Markovic D., Eppenberger P., et. al.: Assessment of median nerve with MR neurography by using diffusion-tensor imaging: normative and pathologic diffusion values. Radiology 2012; 265: pp. 194-203.
23. Leal P.R., Roch J.A., Hermier M., et. al.: Structural abnormalities of the trigeminal root revealed by diffusion tensor imaging in patients with trigeminal neuralgia caused by neurovascular compression: a prospective, double-blind, controlled study. Pain 2011; 152: pp. 2357-2364.
24. Toyone T., Takahashi K., Kitahara H., et. al.: Visualisation of symptomatic nerve roots. Prospective study of contrast-enhanced MRI in patients with lumbar disc herniation. J Bone Joint Surg Br 1993; 75: pp. 529-533.
25. Kobayashi S., Yoshizawa H., Hachiya Y., et. al.: Vasogenic edema induced by compression injury to the spinal nerve root. Distribution of intravenously injected protein tracers and gadolinium-enhanced magnetic resonance imaging. Spine (Phila Pa 1976) 1993; 18: pp. 1410-1424.
26. Pierpaoli C., Barnett A., Pajevic S., et. al.: Water diffusion changes in Wallerian degeneration and their dependence on white matter architecture. Neuroimage 2001; 13: pp. 1174-1185.
27. Bennett I.J., Madden D.J., Vaidya C.J., et. al.: Age-related differences in multiple measures of white matter integrity: a diffusion tensor imaging study of healthy aging. Hum Brain Mapp 2010; 31: pp. 378-390.
28. Morisaki S., Kawai Y., Umeda M., et. al.: In vivo assessment of peripheral nerve regeneration by diffusion tensor imaging. J Magn Reson Imaging 2011; 33: pp. 535-542.
29. Pfefferbaum A., Sullivan E.V.: Increased brain white matter diffusivity in normal adult aging: relationship to anisotropy and partial voluming. Magn Reson Med 2003; 49: pp. 953-961.
30. Maier S.E., Mamata H.: Diffusion tensor imaging of the spinal cord. Ann NY Acad Sci 2005; 1064: pp. 50-60.
31. Yao L., Gai N.: Median nerve cross-sectional area and MRI diffusion characteristics: normative values at the carpal tunnel. Skeletal Radiol 2009; 38: pp. 355-361.
32. Kabakci N., Gurses B., Firat Z., et. al.: Diffusion tensor imaging and tractography of median nerve: normative diffusion values. AJR Am J Roentgenol 2007; 189: pp. 923-927.
33. Tanitame K., Iwakado Y., Akiyama Y., et. al.: Effect of age on the fractional anisotropy (FA) value of peripheral nerves and clinical significance of the age-corrected FA value for evaluating polyneuropathies. Neuroradiology 2012; pp. 815-821.