
Rationale and Objectives
The aim of this study was to assess the role of diffusion-weighted imaging in predicting progression-free survival in patients with head and neck squamous cell carcinoma (HNSCC) treated with induction chemotherapy.
Materials and Methods
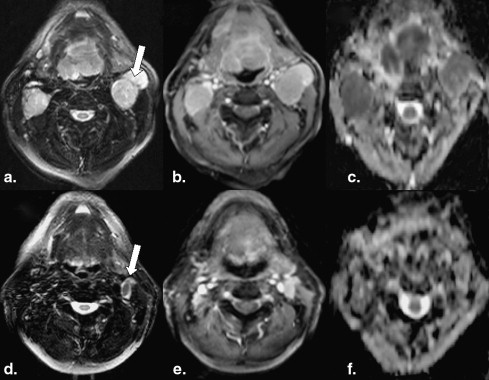
Eighteen patients with HNSCC underwent diffusion-weighted imaging studies prior to treatment and within 3 weeks after completion of induction chemotherapy. Median apparent diffusion coefficient (ADC) values were computed from the largest cervical metastatic lymph node. Percentage changes in ADC values from pretreatment to posttreatment time points were compared between alive and dead patients using the Mann-Whitney U test. P values < .05 were considered statistically significant.
Results
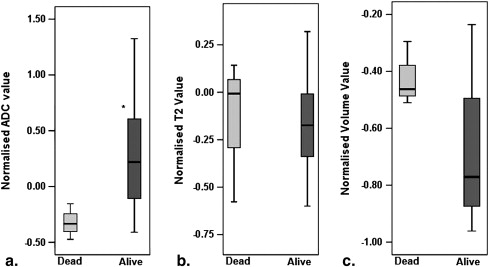
A 22% increase in ADC was observed after induction chemotherapy in alive patients ( n = 15), while patients who died from HNSCC ( n = 3) demonstrated a 33% decrease in ADC. The difference in percentage change in ADC between alive and dead patients was significant ( P = .039).
Conclusions
ADC may be a useful marker in predicting progression-free survival in patients with HNSCC undergoing induction chemotherapy.
Neoadjuvant induction chemotherapy in patients with head and neck squamous cell carcinoma (HNSCC) has resulted in a decline in the risk for distant metastasis and an upsurge in organ preservation . In general, patients responsive to induction chemotherapy also demonstrate positive responses to subsequent radiotherapy . However, given the economic burden and toxic side effects associated with induction chemotherapy in patients with HNSCC , imaging biomarkers that can evaluate treatment and survival outcomes in assessing the efficacy of induction chemotherapy are desirable.
Several physiologic imaging modalities, such as 2-[ 18 F]- fluoro-2-deoxy-D-glucose (FDG) positron emission tomography (PET) , computed tomographic perfusion imaging , proton and phosphorous magnetic resonance spectroscopy , and dynamic contrast-enhanced magnetic resonance imaging (MRI) , have been proposed for predicting and monitoring treatment response as well as predicting survival outcomes in patients with HNSCC undergoing concurrent chemoradiation therapy and surgery. However, lower spatial resolution and specificity associated with FDG-PET, technical limitations associated with performing magnetic resonance spectroscopy, and rigorous steps involved in the analysis of computed tomographic perfusion and dynamic contrast-enhanced MRI data limit the use of these modalities in the routine clinical settings. On the contrary, diffusion-weighted imaging (DWI), which provides maps of microscopic water motion within biologic tissues, offers a more simplistic approach to ascertain physiologic changes within the tumor after treatment. Moreover, relative ease of data acquisition and availability of data processing tools for computing the magnitude of microscopic motion on routine clinical scanners make DWI a more suitable choice.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Patient Population and Treatment
Get Radiology Tree app to read full this article<
Table 1
Characteristics of the Patients
Patient Induction Chemotherapy Protocol Age (y) Gender T N M Dead vs Alive 1 CDDP + TXT + 5-FU 64 M Tx N3 M0 Died of disease 2 CDDP + TXT + 5-FU 55 F T3 N2c M0 Died of disease 3 CDDP + TXT + 5-FU 48 F T4 N2b M0 Died of disease 4 CDDP + TXT + 5-FU 51 M Tx N2b M0 Alive 5 CDBCA + TAX 54 M T3 N2b M0 Alive 6 CDBCA + TAX 63 M T2 N2b M0 Alive 7 CDBCA + TAX + 5-FU 72 M T4 N2c M0 Alive 8 CDDP + TXT + 5-FU 67 M T0 N2b M0 Alive 9 CDDP + TXT + 5-FU 57 M T4 N2c M0 Alive 10 CDDP + TXT + 5-FU 52 M T3 N2c M0 Alive 11 CDDP + TXT + 5-FU 49 M T2 N2c M0 Alive 12 CDDP + TXT + 5-FU 54 M T4 N2c M0 Alive 13 CDDP + TXT + 5-FU 47 M T4 N2b M0 Alive 14 CDDP + TXT + cetuximab 71 M T2 N2a M0 Alive 15 CDDP + TXT + cetuximab 45 M T2 N2b M0 Alive 16 CDDP + TXT + cetuximab 62 M T3 N2b M0 Alive 17 CDDP + TXT + cetuximab 51 M T2 N2b M0 Alive 18 CDDP + TXT + cetuximab 62 M T2 N2c M0 Alive
CDBCA, carboplatin; CDDP, cisplatin; F, female; 5-FU, 5-fluorouracil; M, male; TAX, paclitaxel; TXT, docetaxel.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Data Acquisition
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Image Processing
Get Radiology Tree app to read full this article<
SI(TE)=SI0×exp(−TE/T2). SI
(
TE
)
=
SI
0
×
exp
(
−
TE
/
T
2
)
.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
SIi=SI0×exp(bi×ADC), SI
i
=
SI
0
×
exp
(
b
i
×
ADC
)
,
where SI i is the SI of the diffusion-weighted image at b i .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
(∑numberofpixelsencompassingaregionofinterestfromeachslice)×(slicethickness). (
∑
number
of
pixels
encompassing
a
region
of
interest
from
each
slice
)
×
(
slice
thickness
)
.
Get Radiology Tree app to read full this article<
Clinical Follow-Up and Data Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
percentagechangeinparameter=[(posttreatmentvalueofparameter−pretreatmentvalueofparameter)/pretreatmentvalueofparameter]×100. percentage
change
in
parameter
=
[
(
posttreatment
value
of
parameter
−
pretreatment
value
of
parameter
)
/
pretreatment
value
of
parameter
]
×
100
.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Percentage Changes (Between Pre- and Post Induction Chemotherapy) in Parameters Between Complete Responders and Partial Responders Assessed by Using Different Clinical Endpoints
Clinical Endpoint Percentage Change_P_ Complete Responders Partial Responders ADC Based on 50% reduction in nodal volume 13.7 (−41, 115) 21.2 (−47, 133) .86 At 6 months from the end of all treatment 21.9 (−47, 133) −15.4 (−41, −6) .164 At last follow-up date (December 30, 2010) 23.7 (−35, 115) −15.4 (−47, 133) .113 T2 Based on 50% reduction in nodal volume −27.1 (−60, 32) −37.5 (−58, 14) .126 At 6 months from the end of all treatment −17.4 (−60, 32) −9.1 (−59, −1) .824 At last follow-up date (December 30, 2010) −17.4 (−40, 32) −9.1 (−60, 14) .546 Volume Based on 50% reduction in nodal volume — — — At 6 months from the end of all treatment −77.1 (−96, −24) −51.1 (−77, −41) .498 At last follow-up date (December 30, 2010) −81.1 (−96, −30) −49.6 (−95, −24) .113
Data are expressed as median (minimum, maximum).
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Posner M., Vermorken J.B.: Induction therapy in the modern era of combined-modality therapy for locally advanced head and neck cancer. Semin Oncol 2008; 35: pp. 221-228.
2. Specenier P.M., Vermorken J.B.: Neoadjuvant chemotherapy in head and neck cancer: should it be revisited?. Cancer Lett 2007; 256: pp. 166-177.
3. Ensley J.F., Jacobs J.R., Weaver A., et. al.: Correlation between response to cisplatinum-combination chemotherapy and subsequent radiotherapy in previously untreated patients with advanced squamous cell cancers of the head and neck. Cancer 1984; 54: pp. 811-814.
4. Lee W.C., Chavez Y.E., Baker T., et. al.: Economic burden of heart failure: a summary of recent literature. Heart Lung 2004; 33: pp. 362-371.
5. Fury M.G., Shah J.P.: Induction chemotherapy in the management of head and neck cancer. J Surg Oncol 2010; 101: pp. 292-298.
6. Minn H., Lapela M., Klemi P.J., et. al.: Prediction of survival with fluorine-18-fluoro-deoxyglucose and PET in head and neck cancer. J Nucl Med 1997; 38: pp. 1907-1911.
7. Schwartz D.L., Rajendran J., Yueh B., et. al.: FDG-PET prediction of head and neck squamous cell cancer outcomes. Arch Otolaryngol Head Neck Surg 2004; 130: pp. 1361-1367.
8. Hermans R., Meijerink M., Van den Bogaert W., et. al.: Tumor perfusion rate determined noninvasively by dynamic computed tomography predicts outcome in head-and-neck cancer after radiotherapy. Int J Radiat Oncol Biol Phys 2003; 57: pp. 1351-1356.
9. Gandhi D., Hoeffner E.G., Carlos R.C., et. al.: Computed tomography perfusion of squamous cell carcinoma of the upper aerodigestive tract. Initial results. J Comput Assist Tomogr 2003; 27: pp. 687-693.
10. Maldonado X., Alonso J., Giralt J., et. al.: 31Phosphorus magnetic resonance spectroscopy in the assessment of head and neck tumors. Int J Radiat Oncol Biol Phys 1998; 40: pp. 309-312.
11. Shukla-Dave A., Poptani H., Loevner L.A., et. al.: Prediction of treatment response of head and neck cancers with P-31 MR spectroscopy from pretreatment relative phosphomonoester levels. Acad Radiol 2002; 9: pp. 688-694.
12. Bezabeh T., Odlum O., Nason R., et. al.: Prediction of treatment response in head and neck cancer by magnetic resonance spectroscopy. AJNR Am J Neuroradiol 2005; 26: pp. 2108-2113.
13. Kim S., Loevner L.A., Quon H., et. al.: Prediction of response to chemoradiation therapy in squamous cell carcinomas of the head and neck using dynamic contrast-enhanced MR imaging. AJNR Am J Neuroradiol 2010; 31: pp. 262-268.
14. Gupta R.K., Sinha U., Cloughesy T.F., et. al.: Inverse correlation between choline magnetic resonance spectroscopy signal intensity and the apparent diffusion coefficient in human glioma. Magn Reson Med 1999; 41: pp. 2-7.
15. Guo A.C., Cummings T.J., Dash R.C., et. al.: Lymphomas and high-grade astrocytomas: comparison of water diffusibility and histologic characteristics. Radiology 2002; 224: pp. 177-183.
16. Zhao M., Pipe J.G., Bonnett J., et. al.: Early detection of treatment response by diffusion-weighted 1H-NMR spectroscopy in a murine tumour in vivo. Br J Cancer 1996; 73: pp. 61-64.
17. Chenevert T.L., McKeever P.E., Ross B.D.: Monitoring early response of experimental brain tumors to therapy using diffusion magnetic resonance imaging. Clin Cancer Res 1997; 3: pp. 1457-1466.
18. Poptani H., Puumalainen A.M., Grohn O.H., et. al.: Monitoring thymidine kinase and ganciclovir-induced changes in rat malignant glioma in vivo by nuclear magnetic resonance imaging. Cancer Gene Ther 1998; 5: pp. 101-109.
19. Kauppinen R.A.: Monitoring cytotoxic tumour treatment response by diffusion magnetic resonance imaging and proton spectroscopy. NMR Biomed 2002; 15: pp. 6-17.
20. Hamstra D.A., Lee K.C., Moffat B.A., et. al.: Diffusion magnetic resonance imaging: an imaging treatment response biomarker to chemoradiotherapy in a mouse model of squamous cell cancer of the head and neck. Transl Oncol 2008; 1: pp. 187-194.
21. Sumi M., Sakihama N., Sumi T., et. al.: Discrimination of metastatic cervical lymph nodes with diffusion-weighted MR imaging in patients with head and neck cancer. AJNR Am J Neuroradiol 2003; 24: pp. 1627-1634.
22. Wang J., Takashima S., Takayama F., et. al.: Head and neck lesions: characterization with diffusion-weighted echo-planar MR imaging. Radiology 2001; 220: pp. 621-630.
23. Srinivasan A., Dvorak R., Perni K., et. al.: Differentiation of benign and malignant pathology in the head and neck using 3T apparent diffusion coefficient values: early experience. AJNR Am J Neuroradiol 2008; 29: pp. 40-44.
24. Razek A.A., Megahed A.S., Denewer A., et. al.: Role of diffusion-weighted magnetic resonance imaging in differentiation between the viable and necrotic parts of head and neck tumors. Acta Radiol 2008; 49: pp. 364-370.
25. Vandecaveye V., De Keyzer F., Nuyts S., et. al.: Detection of head and neck squamous cell carcinoma with diffusion weighted MRI after (chemo)radiotherapy: correlation between radiologic and histopathologic findings. Int J Radiat Oncol Biol Phys 2007; 67: pp. 960-971.
26. Abdel Razek A.A., Kandeel A.Y., Soliman N., et. al.: Role of diffusion-weighted echo-planar MR imaging in differentiation of residual or recurrent head and neck tumors and posttreatment changes. AJNR Am J Neuroradiol 2007; 28: pp. 1146-1152.
27. Kim S., Loevner L., Quon H., et. al.: Diffusion-weighted magnetic resonance imaging for predicting and detecting early response to chemoradiation therapy of squamous cell carcinomas of the head and neck. Clin Cancer Res 2009; 15: pp. 986-994.
28. Kato H., Kanematsu M., Tanaka O., et. al.: Head and neck squamous cell carcinoma: usefulness of diffusion-weighted MR imaging in the prediction of a neoadjuvant therapeutic effect. Eur Radiol 2009; 19: pp. 103-109.
29. King A.D., Mo F.K., Yu K.H., et. al.: Squamous cell carcinoma of the head and neck: diffusion-weighted MR imaging for prediction and monitoring of treatment response. Eur Radiol 2010; 20: pp. 2213-2220.
30. Vandecaveye V., Dirix P., De Keyzer F., et. al.: Predictive value of diffusion-weighted magnetic resonance imaging during chemoradiotherapy for head and neck squamous cell carcinoma. Eur Radiol 2010; 20: pp. 1703-1714.
31. Garden A.S., Asper J.A., Morrison W.H., et. al.: Is concurrent chemoradiation the treatment of choice for all patients with stage III or IV head and neck carcinoma?. Cancer 2004; 100: pp. 1171-1178.
32. Denis F., Garaud P., Bardet E., et. al.: Final results of the 94–01 French Head and Neck Oncology and Radiotherapy Group randomized trial comparing radiotherapy alone with concomitant radiochemotherapy in advanced-stage oropharynx carcinoma. J Clin Oncol 2004; 22: pp. 69-76.
33. Galons J.P., Altbach M.I., Paine-Murrieta G.D., et. al.: Early increases in breast tumor xenograft water mobility in response to paclitaxel therapy detected by non-invasive diffusion magnetic resonance imaging. Neoplasia 1999; 1: pp. 113-117.
34. Sharma U., Danishad K.K., Seenu V., et. al.: Longitudinal study of the assessment by MRI and diffusion-weighted imaging of tumor response in patients with locally advanced breast cancer undergoing neoadjuvant chemotherapy. NMR Biomed 2009; 22: pp. 104-113.
35. Yoshida S., Koga F., Kawakami S., et. al.: Initial experience of diffusion-weighted magnetic resonance imaging to assess therapeutic response to induction chemoradiotherapy against muscle-invasive bladder cancer. Urology 2010; 75: pp. 387-391.
36. Chepeha D.B., Sacco A.G., Oxford L.E., et. al.: Advanced squamous cell carcinoma of the oropharynx: efficacy of positron emission tomography and computed tomography for determining primary tumor response during induction chemotherapy. Head Neck 2009; 31: pp. 452-460.
37. Chu E., DeVita V.T.: Principles of medical oncology.DeVita V.T.Hellman S.Rosenberg S.A.Cancer: Principles & Practice of Oncology.2005.Lippincott Williams & WilkinsPhiladelphia, PA:pp. 296-306.
38. Larocque M.P., Syme A., Yahya A., et. al.: Monitoring T2 and ADC at 9.4 T following fractionated external beam radiation therapy in a mouse model. Phys Med Biol 2010; 55: pp. 1381-1393.
39. Larocque M.P., Syme A., Yahya A., et. al.: Temporal and dose dependence of T2 and ADC at 9.4 T in a mouse model following single fraction radiation therapy. Med Phys 2009; 36: pp. 2948-2954.
40. Madhu B., Waterton J.C., Griffiths J.R., et. al.: The response of RIF-1 fibrosarcomas to the vascular-disrupting agent ZD6126 assessed by in vivo and ex vivo 1H magnetic resonance spectroscopy. Neoplasia 2006; 8: pp. 560-567.
41. Knegjens J.L., Hauptmann M., Pameijer F.A., et. al.: Tumor volume as prognostic factor in chemoradiation for advanced head and neck cancer. Head Neck 2011; 33: pp. 375-382.
42. Brenner D.J.: Dose, volume, and tumor-control predictions in radiotherapy. Int J Radiat Oncol Biol Phys 1993; 26: pp. 171-179.
43. Bentzen S.M., Ruifrok A.C., Thames H.D.: Repair capacity and kinetics for human mucosa and epithelial tumors in the head and neck: clinical data on the effect of changing the time interval between multiple fractions per day in radiotherapy. Radiother Oncol 1996; 38: pp. 89-101.
44. Dubben H.H., Thames H.D., Beck-Bornholdt H.P.: Tumor volume: a basic and specific response predictor in radiotherapy. Radiother Oncol 1998; 47: pp. 167-174.
45. Wendt T.G., Bank P.: Prognostic factors in squamous cell carcinoma of the head and neck. Onkologie 2002; 25: pp. 208-212.
46. Forastiere A.A., Ang K., Brizel D., et. al.: Head and neck cancers. J Natl Compr Canc Netw 2005; 3: pp. 316-391.