
Rationale and Objectives
To evaluate the correlation between apparent diffusion coefficient (ADC) values of the pancreas on diffusion-weighted imaging (DWI) and pancreatic exocrine function determined by HCO 3 concentration in the secretin endoscopic pancreatic function test (ePFT).
Materials and Methods
Mean ADC values derived from 10 different points of the pancreatic gland on DWI were reviewed in 14 patients with normal (peak HCO 3 ≥80 mEq/L) and 14 patients with abnormal (peak HCO 3 <80 mEq/L) ePFT results. Magnetic resonance cholangiopancreatography (MRCP) images of the same patients were evaluated for the diagnosis of chronic pancreatitis. Correlation between ADC values and HCO 3 concentration as well as Cambridge scores in MRCP was performed using Spearman’s correlation test.
Results
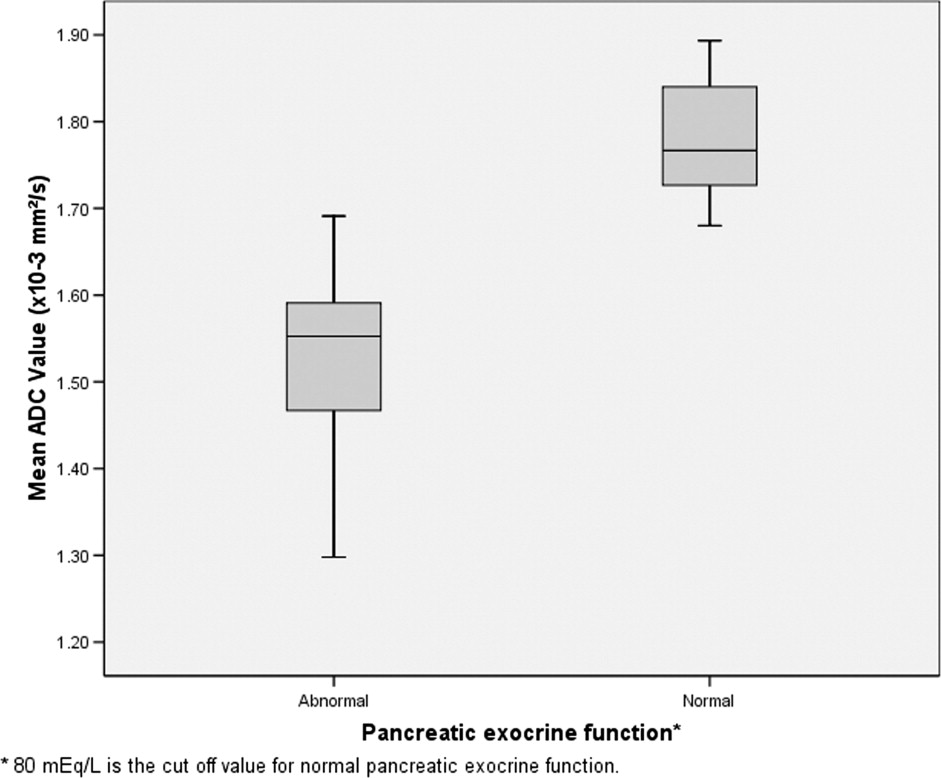
Mean ADC value of the pancreas was 1.52 ± 0.13 × 10 −3 mm 2 /s in patients with abnormal ePFT results and 1.78 ± 0.07 × 10 −3 mm 2 /s in the normal group. There was a significant statistical difference between the ADC values of the pancreas in the two groups ( P < .0001). There was also a statistically significant correlation between HCO 3 level and ADC value of the pancreas in the study patients ( r = 0.771, P < .0001). Morphologic changes of the pancreas according to the Cambridge classification were also well correlated with the mean ADC values ( r = −0.763, P < .0001).
Conclusions
Strong correlation between ADC value and pancreatic exocrine function as well as Cambridge score for chronic pancreatitis exists. Further studies are needed to determine the cut off ADC value for chronic pancreatitis.
Pancreatic exocrine function testing is considered a clinical marker for the evaluation of chronic pancreatitis ( ). On imaging, the Cambridge classification system has been used to determine morphologic severity of chronic pancreatitis ( ). Although the Cambridge classification system correlates well with the clinical parameters of chronic pancreatitis, there are overlapping findings and inconclusive cases are not uncommon ( ). Therefore, a parametric marker on imaging may be helpful for the evaluation of chronic pancreatitis and monitoring patients for the severity of the disease. Diffusion-weighted magnetic resonance imaging (MRI) is characterized by intravoxel incoherent motion imaging of H + protons that can assess molecular diffusion and microcirculation of the blood in the capillary network of biologic tissues ( ). A recent study has shown the use of diffusion-weighted imaging (DWI) for the diagnosis of chronic pancreatitis after secretin stimulation in alcoholics ( ). In this study, we retrospectively reviewed apparent diffusion coefficient (ADC) values of patients with an abnormal secretin endoscopic pancreatic function test (ePFT) and compared them with those who had a normal ePFT and with the magnetic resonance cholangiopancreatography (MRCP) findings of chronic pancreatitis based on the Cambridge classification system.
Materials and methods
Patients
This study was performed retrospectively and is Health Insurance Portability and Accountability Act–compliant. The institutional review board approved the study and waived the requirement for informed consent for our patient data review. Retrospective review of patients’ charts revealed 28 consecutive patients (3 males, 25 females; ages 32–67 years, mean 48.6) who had undergone MRCP and ePFT within a 1- to 4-week interval. Patients were referred for MRCP with upper abdominal pain to rule out underlying hepatobiliary disease. ePFT was performed in cases with 1) normal MRCP findings and clinically suspected pancreatitis and 2) suspected or definite MRCP diagnosis of chronic pancreatitis.
Imaging
Get Radiology Tree app to read full this article<
Secretin ePFT
Get Radiology Tree app to read full this article<
Image Analysis
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Functional and Imaging Findings in Patients with Normal and Abnormal ePFT Results
Normal ePFT Abnormal ePFT ePFT ⁎ Cambridge † Mean ADC ‡ ePFT ⁎ Cambridge † Mean ADC ‡ 92 0 1.82 32 4 1.26 95 0 1.76 38 1 1.30 96 0 1.89 50 1 1.63 102 0 1.75 57 0 1.59 104 0 1.69 59 3 1.52 105 0 1.85 62 1 1.58 109 0 1.73 63 1 1.55 110 0 1.84 73 3 1.56 111 0 1.68 74 1 1.61 112 0 1.77 77 0 1.47 116 0 1.83 77 1 1.53 142 0 1.73 78 1 1.59 160 0 1.72 78 1 1.40 173 0 1.89 79 1 1.69
ADC: apparent diffusion coefficient; ePFT: endoscopic pancreatic function test.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Chowdhury R.S., Forsmark C.E.: Review article: pancreatic function testing. Aliment Pharmacol Ther 2003; 17: pp. 733-750.
2. Boeck W.G., Adler G., Gress T.M.: Pancreatic function tests: when to choose, what to use. Current Gastroenterol Rep 2001; 3: pp. 95-100.
3. Axon A.T., Classen M., Cotton P.B., et. al.: Pancreatography in chronic pancreatitis: international definitions. Gut 1984; 25: pp. 1107-1112.
4. Pungpapong S., Wallace M.B., Woodward T.A., et. al.: Accuracy of endoscopic ultrasonography and magnetic resonance cholangiopancreatography for the diagnosis of chronic pancreatitis. J Clin Gastroenterol 2007; 41: pp. 88-93.
5. Tamura R., Ishibashi T., Takahashi S.: Chronic pancreatitis: MRCP versus ERCP for quantitative caliber measurement and qualitative evaluation. Radiology 2006; 238: pp. 920-928.
6. Le Bihan D., Breton E., Lallemand D., et. al.: Separation of diffusion and perfusion in intravoxel incoherent motion MR imaging. Radiology 1998; 168: pp. 497-505.
7. Yamada I., Aung W., Himeno Y., et. al.: Diffusion coefficients in abdominal organs and hepatic lesions: evaluation with intravoxel incoherent motion echo-planar MR imaging. Radiology 1999; 210: pp. 617-623.
8. Erturk S.M., Ichikawa T., Motosugi U., et. al.: Diffusion-weighted MR imaging in the evaluation of pancreatic exocrine function before and after secretin stimulation. Am J Gastroenterol 2006; 101: pp. 133-136.
9. Dominguez-Munoz J.E.: Clinical pancreatology for practicing gastroenterologists and surgeons.2006.Blackwell PublishingMalden, MA
10. Otsuki M.: Chronic pancreatitis. Pancreatology 2004; 4: pp. 28-41.
11. Takehara Y., Ichijo K., Tooyama N., et. al.: Breath-hold MR cholangiopancreatography with a long-echo-train fast spin-echo sequence and a surface coil in chronic pancreatitis. Radiology 1994; 192: pp. 73-78.
12. Sica G.T., Braver J., Cooney M.J., et. al.: Comparison of endoscopic retrograde cholangiopancreatography with MR cholangiopancreatography in patients with pancreatitis. Radiology 1999; 210: pp. 605-610.
13. Malfertheiner P., Buchler M., Stanescu A., et. al.: Exocrine pancreatic function in correlation to ductal and parenchymal morphology in chronic pancreatitis. Hepatogastroenterology 1986; 33: pp. 110-114.
14. Semelka R.C., Ascher S.M.: MR imaging of the pancreas. Radiology 1993; 188: pp. 593-602.
15. Balci N.C., Alkaade S., Akduman I.E., et. al.: Serial contrast-enhanced MRI of the pancreas: correlation with secretin-stimulated endoscopic pancreatic function test. Acad Radiol 2006; 13: pp. 1367-1372.
16. Thoeny H.C., De Keyzer F.: Extracranial applications of diffusion-weighted magnetic resonance imaging. Eur Radiol 2007; 17: pp. 1385-1393.
17. Koh D.M., Collins D.J.: Diffusion-weighted MRI in the body: applications and challenges in oncology. Am J Roentgenol 2007; 188: pp. 1622-1635.
18. Girometti R., Furlan A., Bazzocchi M., et. al.: Diffusion-weighted MRI in evaluating liver fibrosis: a feasibility study in cirrhotic patients. Radiol Med 2007; 12: pp. 394-408.
19. Koinuma M., Ohashi I., Hanafusa K., et. al.: Apparent diffusion coefficient measurements with diffusion-weighted magnetic resonance imaging for evaluation of hepatic fibrosis. J Magn Reson Imaging 2005; 22: pp. 80-85.
20. Ichikawa T., Haradome H., Hachiya J., et. al.: Diffusion-weighted MR imaging with single-shot echo-planar imaging in the upper abdomen: preliminary clinical experience in 61 patients. Abdom Imaging 1999; 24: pp. 456-461.